
Psychoanalyst Toby Ingham reflects on the emotional impact of his psychotherapy client’s premature termination.
Think Act Be: A Whole Person Approach to Healing

Psychotherapist Seth Gillihan’s CBT Deck helps clients to think, act and be on their road to healing.
Qualia and Quiddities in Psychotherapy

Clinician and researcher Margaret Arnd-Caddigan stands at the edge of the scientific method and wonders if science might just undermine good therapy.
How to Master the Art of Developing Your Therapeutic Voice

Effective psychotherapy requires that the clinician find their true voice, much like the artists’ journey.
Psychotherapy and Autism

Psychotherapist Daniel Marston helps us to better understand the unique treatment needs of young adults on the autism spectrum.
My First Private Patient
As a young therapist, Valery Hazanov reflects on his therapeutic relationship with an elder fellow Russian, and wonders if he made a difference.
The Tiger Woods Analogy for Therapists Makes a Roaring Comeback!

Watching Tiger Woods from the gallery on the 18th hole of the Masters Tournament, Howard Rosenthal has advice for psychotherapists.
Unlearning to Learn

Clinicians Pooja Gala and Urvi Paralkar reflect on the challenges of unlearning cherished notions about therapy in order to be fully present for their clients.
Circle of Development: How Clinical Supervisors Can Help You Get to Your Growth Edge
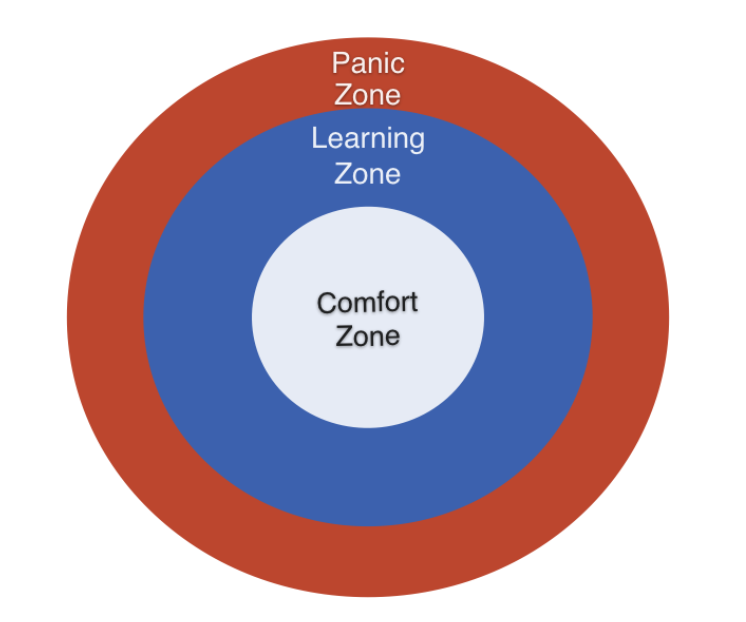
In his second installment on clinical supervision, Daryl Chow suggests ways to help supervisees move beyond their comfort zone in order to improve clinical outcomes.
The Murder of Hope

Relatively new to her career as a psychotherapist, Kayla Rees mourns the loss of a young client to suicide.