Becoming an Artist
Surrounded by a sea of attendees at Psychotherapy Networker’s annual conference, I waited to ask my hero the question that had been burning inside. One man, with an uncanny resemblance to Sigmund Freud, entranced us yet again with a story of the work we’d all been celebrating and emulating in our own offices for so many years. Our master clinician and storyteller, group therapy guru, and most importantly, the single most generous and open discloser of his clinical process, Irvin Yalom was reflecting on his lifetime contributions.
It was now our turn to ask him questions. “Dr. Yalom, you’ve shown us how to embrace the process, and as the poet Rilke advised, to: ‘be patient toward all that is unsolved in your heart and try to love the questions themselves.’” Was I even talking into the microphone? The notes on my phone bounced out of focus, but I pressed on.
“Like jazz musicians, you’ve reminded us to enjoy the dissonances and savor the surprises we find within them. Can you talk about that, the role and importance of being an artist in our field?” I was grateful when he acknowledged that yes, he had thought of calling his book Letters to a Young Therapist after Rilke’s famous missives. “Even though I idolized so many, no, no, I never thought of myself as an artist. Even though I had wanted to be one, it wasn’t me!” It was like I had framed the wrong man. With him ready to quickly move on, I was stunned, stung, crestfallen. If Yalom couldn’t recognize being an artist, how could any of us?
Luckily for me — and us — Sue Johnson, the puckish British couples therapist and our evening’s interviewer, held him up a minute to take stock of his knee-jerk demurral. Wasn’t his work — its graceful storytelling and open embrace of the therapeutic process a testament to the power of our art to heal and enlarge? Was this any less artistic than the poet, musician, or actor’s craft?
Yalom’s initial objection ripened into delight on stage, and after the conference, in a private email, he thanked me, stating simply, “I’ll remember your comment for a very, very long time.” That’s what this essay is about: the artistry of our work and how we develop a therapeutic voice to help us get there. This is vital not only for ourselves and our supervisees, but even more so for our clients, who cultivate their own voice in the interplay with ours. Happily, there is ample scientific and empirical support for this artistic venture and cultivation of the voice, and I will use it to contextualize and illuminate our journey along the way.
Finding Our Voice
All artists — whether writers, musicians, or actors — must develop a voice, that hard-to-define yet distinctive style which runs like an invisible thread through their work, opening a space of creative possibility between their art and audience. As a supervisor of beginning therapists, I view this as essential, and liken it to the process we see on television each week on the show “The Voice.”
Just as Kelly Clarkson, Blake Shelton, and Adam Levine compassionately and thoughtfully mold, mentor, and inspire young talent, so too must we as supervisors help our beginning clinicians. Each has their own music and style they come in playing, and supervisors help them draw out their raw talent, experiment with new genres, and ultimately learn about how to make music that is, as Duke Ellington said, “beyond category.” This is therapy that transcends theoretical orientations, becoming a unique blend of the clinician’s theoretical and empirical knowledge, their personality, and emerging therapeutic repertoire.
There is a yin and yang here that, when in proper balance and harmony, lead to a fully developed artistic voice. This voice not only serves the therapist but promotes the opening and expansion of the patient’s own voice, becoming the driving force of creative therapeutic work. This also forms the basis for a lifetime of creating art. Yes, all of us therapists (veterans too!) do this daily, in the poetic and musical lines we shape in what others easily pass over as ordinary prose. Freud had it right from the beginning when he suggested, “When we can share that is poetry in the prose of life.”
Wouldn’t it be inspiring if all of us — beginning and veteran clinicians alike, supervisors and supervisees — could embrace the artistry of our everyday work? Wouldn’t it be illuminating if we had a working model of how to cultivate and deepen this?
Building a Voice
The model that I’ve arrived at is both simple yet expansive. A therapeutic voice is the combination and interplay of therapeutic presence and therapeutic authority, the complementary and seemingly contradictory elements that like yin and yang, enable us to create a three-dimensional picture of our patients and ourselves. Think of it like how our two eyes, each with their independent perspectives, magically create depth perception.
An ambitious supervisee recently confessed to me, “I have to anticipate everything before our session, and know exactly where I am taking my clients. I feel like a white-water rafting guide who’s one turn away from taking the whole crew down with me!”
This supervisee, like so many others, is proficient at being directive, setting goals, and moving quickly towards intervention. Unfortunately, they don’t offer enough room for the patient to openly explore and steep in their feelings or draw on the relational process to entertain new possibilities, which is why they so often feel up a creek without a paddle.
Therapeutic Presence
What they need more of is the yin of therapeutic voice, therapeutic presence — the capacity to be receptive, mindfully attentive, emotionally available, nonjudgmental and resonant with the client’s unfolding experience (1). Freud originated this concept in his earliest recommendation for practicing therapists in 1912, underscoring the vital importance of “evenly hovering attention.” Like a koan, the therapist should “simply listen and not bother about whether he is keeping anything in mind.”
Considered the foundation for tuning in to the patient’s unconscious, it provided a potent tool for opening one’s mind and heart to new possibilities for understanding and engaging the patient’s psyche. Like the Zen Buddhist notion of “beginner’s mind,” or mindfulness itself, therapeutic presence comes from the framework of “not knowing” in the service of creativity. To paraphrase the Nobel prize-winning poet Wislawa Szymborska, the point — like the poet’s main task — is to say I don’t know and keep on going. It’s to wonder aloud!
Therapeutically present therapists are understanding, open-minded, and comfortable with a range of different feelings and perspectives.These therapists have internalized Robert Frost’s prescient quip, “No surprise for the writer. No surprise for the reader!” Patients feel a sense of safety, trust, and warmth in their company. The space seems to open with them. This disarming quality makes it easy for patients to explore new subplots and turns in their stories. They find themselves surprised at how much they are saying and learning in just the telling itself.
Therapists who practice this kind of presence don’t have to know immediately and aren’t bothered by the ambiguity or complexity of what they are hearing; they “dwell in possibility,” as Emily Dickinson said, a “fairer house than prose.” They allow patients to be in the driver’s seat so that they can show them the territory first, and in so doing, instruct their therapist how to best be of service. This openness allows patients to take more risks in therapy, to deepen the exploration of their thoughts and feelings, and to get to genuinely enjoy the deeper waters of the psyche, even providing modeling for them to be more open to the various and contradictory sides of themselves! In short, to paraphrase Whitman, they are reminded that, “We are large. We contain multitudes!”
Owning A Voice
Plopping down in my office chair, and letting out a formidable sigh, another supervisee recently lamented: “Sometimes I feel like I’m taking it all in but then can’t get a word in edgewise, and I’m not even sure if what I’m thinking even makes sense. Am I really helping them at all, or are my own mixed-up feelings just getting in the way of making any headway?”
I know many fantastic supervisees who excel at being empathic, reflective, and thoughtful with their patients, but lack the confidence to make discriminating interpretations that take into account their valuable instincts and intuition regarding new creative possibilities.
These supervisees, understandably, worry that if they use too much of their authority, they will overwhelm or possibly hurt their clients.
They need more of the yang of the voice of therapeutic authority — which I define as the command of theory and technique and a discriminating awareness of how to put these into practice. It is the confidence to properly select, apply, time, and adjust one’s interventions in a multicultural and relationally sensitive manner (by relying on the yin of therapeutic presence, of course!).
The clinician with therapeutic authority is happy to show patients how to blaze a new trail and empower them to sort through the various aspects of their experience to find bigger patterns and new possibilities. Like an artist mentoring a new student, they can see the bigger and smaller picture and can help with the difficult passages encountered in putting new skills and pieces together. Most importantly, the therapist with a balanced dose of therapeutic authority knows how to do this with proper timing, tact and empathy. They are not going to break patients down like a military drill sergeant, but instead are going to be thoughtfully discriminating and penetrate deeper into problems and their implied solutions.
Supervisory Support
It is vital for supervisors to support beginning clinicians in developing their clinical intuition and instincts, the confident application of their theoretical and empirical knowledge, and a sense for having the “authority” to make therapeutic moves. Just as a singer needs to take risks with trying out new ways to expand their interpretation of a song, so too does the beginning clinician, and as supervisors, we are right behind them to encourage it!
Supervisors also need to model how to both be comfortable with and to chase the kind of not-knowing that makes creative therapeutic work possible. Like Yoda to Luke Skywalker, we help emerging clinicians to learn how to use “The Force,” showing them that, paradoxically, it is only by surrendering and letting go that we truly open the space for something new to emerge.
Just like our young poet needed Rilke to learn how to become an artist (and Rilke in turn was mentored by the great sculptor Auguste Rodin), so too do our beginning clinicians need us to illustrate how they can be balanced and integrated in their own unique therapeutic voice by uniting these two crucial faculties. And it turns out that all of us, no matter what level we are at, need to remember that we are always cultivating and expressing this artistry!
Empirically Supported Artistry
Art never needs more than its own justification, but as a scientist practitioner, you might need to be reminded of the scientific support for viewing therapy as an artistic enterprise. Look no further than Neuroscientist Antonio Damasio’s recent book, The Strange Order of Things, which eloquently showcases the way in which our “right-brained” feeling comes first, inspiring and motivating our greatest cultural innovations and products, and that joined together with the logic and language of our left-brains, becomes something truly extraordinary. Daniel Pink in In a Whole New Mind illustrates the 21st century’s cultural sea change from a left-brained leaning computer age, to a right-brained leaning conceptual age that integrates right and left to make the best of both worlds.
In my model, therapeutic presence is the right-brain dominant aspect of our therapeutic artistry, and therapeutic authority is the left-brain pilot, so to speak. Therapeutic presence is at once dreamlike and free-associative, holistic and big-picture, image and metaphor centered, and largely implicit and nonverbal. It undergirds the profound empathic connection between us and our patients, especially to those sides of our clients that have experienced trauma and yet still long for—even in secret — a more redemptive narrative.
Therapeutic authority flows from the language and logic-based sides of our brain with its highly developed executive functioning. More largely conscious and deliberate, this side enables us to zero in and edit the many clinical possibilities before us so that we can work with true specificity and discernment, tailoring our treatment for the unique person sitting across from us, and getting to the heart of the matter.
A 19th century poem by Frances Cornford sums up this lovely process best. Entitled “The Guitarist Tunes Up”, we learn that this musician leans into their instrument with ‘attentive courtesy’:
Not as a lordly conqueror who could
Command both wire and wood,
But as a man with a loved woman might,
Inquiring with delight
What slight essential things she had to say
Before they started, he and she, to play.
For a visual of this interplay, we can look to none other than that famous Renaissance man — Da Vinci and his iconic drawing of his Vitruvian Man. It is only by integrating the square of our logic with the circle of our feeling do we become something truly divine — artists in our own right.
Learning & Teaching from Art
If we are to find and develop a therapeutic voice, we must first look at how therapy itself connects to the arts and how, as supervisors and supervisees, we can attend to these important dimensions. We’ll look specifically to poetry and music as starting points.
Poetry Lessons
A poem, such as a sonnet, compresses a question or problem, its exploration, and a final statement of some revelation or new understanding into 14 lines. In Shakespeare’s famous sonnet, “Shall I compare thee to a summer’s day?” the speaker wrestles back and forth with how his love is and is not like summer. Initially, it seems very fitting to compare her to the beauty and splendor of the season, but upon further inspection, new ideas emerge. Among other things, she is much more constant, evenly tempered, reliable, and more lovely than the summer months.
Much like Shakespeare’s speaker, we wrestle with our initial diagnostic impressions of our patients: Shall I compare thee to a borderline personality, a depressive, or an adjustment disorder? It is not immediately clear, and so many of our first sessions entail testing out various hypotheses to determine who the patient is and is not.
As Shakespeare’s poem continues, surprises and new discoveries emerge and toward the final turn of the poem, the poet concludes that his love will be eternal as a result of the poetic act itself: “So long as men can breathe or eyes can see/so long lives this, and this gives life to thee.” This is the aim of a transformative therapeutic process. Much like a sonnet, by the end of the therapeutic experience, a patient will be able to make a few “turns” and come to a way of internalizing the therapeutic process so that it too will become eternal.
Music Lessons
Beethoven’s fifth symphony provides an immediately recognizable compressed musical idea. In only four notes, a focal theme is established that is explored, varied, and reharmonized much in the same way that occurs in therapy. The capacity of the therapist to articulate that melody — the dominant trend or relational pattern that pulls the various strands of a patient’s story together —goes very far in clarifying what has been troubling patients while it points them in the direction of how they can move forward. Much of the time, patients are playing the notes of their issues but are not aware of the melody and cannot synthesize it into a focal theme. They bring us their own invisible scores and hope we will give them feedback to recognize their own music.
About seven and a half minutes into the third movement of Rachmaninov’s Symphony in E minor, we hear the main theme played by the French horn, in the manner that a patient initially expresses when it is recognized by the counselor: “You hear me! This is the song I didn’t know I was singing.” Shortly after, the theme gets played by the violin with a melancholy poignancy: “I have been waiting a long time suffering with this alone.” This is the sense of sadness and mourning that the patient feels for having had to sequester this aspect of self in the service of protection and adaptation.
As the theme gets worked upon and elaborated, new instruments, such as the oboe and flute, come in to take on the line, with hope gathering. Calmer and with greater poise, a certain pride and expressiveness opens now that this very significant idea can be incorporated into the larger musical narrative of the patient’s story.
Let’s see how this artistry translates to a representative case and get a preview of putting all the pieces together.
A Case of You
I’ve named this “A Case of You” as a nod to Joni Mitchell’s heartbreakingly beautiful song because this patient seemed at first blush like she was too much to handle. Pretty quickly into our first session, I realized that, like for so many of our cases, the following lyrics truly applied:
“You’re in my blood, you’re my holy wine, you’re so bitter and so sweet, oh I could drink a case of you, and I’d still be on my feet!”
A student came to her intake appointment complaining that her friends did not understand her, that she couldn’t fathom why they were so turned off by the razor blade that she kept on her desk as a reminder that she could cut herself, and that she had been told to come to counseling many times, but it had never been helpful in the past. She asked, why should she bother now?
Previous counselors told her that she needed a higher level of care than they could provide, and those appointments left the student feeling misunderstood and blamed for troubles she could not fathom. She also felt a sense of hopelessness at not being able to make true contact, just as she had not with family and friends. Aiming right for the jugular, she also scoffed at me: “Counselors are incompetent and don’t really understand me. You probably won’t either!”
In addition to feeling interpersonally rejected on several fronts, as a first-generation college student, she experienced the pressure of well-meaning parents who hoped to see the family’s metaphorical stock rise with her success. At the same time, her family expected her to be at the ready when they called her to take care of her younger siblings. She was a painter who loved the darkest colors of her palette, with her works centering on Hopperesque misfits wandering in the night.
Initially, her cutting was a regular strategy to express and modulate her emotions, combined with a preoccupation with death, and the ways in which friends and other therapists had been repelled by her behavior made me wonder whether this student had borderline personality disorder. Like in Shakespeare’s poem, though, I was not sure whether this comparison truly fit.
Here we see the internal wrestling of therapeutic authority and presence. The first stab at therapeutic authority can have us all too quickly categorize or even pathologize what we are seeing before we get the full story. At the same time, this discriminating faculty provides crucial information that we really need to follow. Like a samurai warrior, psychologically speaking we need to forge the sword and learn how to use it appropriately. Toggling back and forth between this function and therapeutic presence — the open and receptive Buddha nature — allows us to see the big picture clearly while also focusing keenly on the supporting details that we need to assess and intervene incisively.
As I got to know more about the patient’s relational backdrop and leaned into my therapeutic presence, things looked a bit different. I learned about her parents’ difficulty tolerating fear, anger, and sadness, and their own struggles with managing chronically high levels of stress. I also learned about my client’s repeated experiences of the family being unable to acknowledge or stay with her emotional experience.
Just as the subject of the Shakespearian poem was no longer so much like the summer, it seemed more and more that she was no longer like a patient with a borderline organization and instead more like one with a neurotic organization or a possible adjustment disorder. She appeared to be in a conflict that could not be acknowledged squarely as she was in the midst of an important developmental transition, both issues coloring each other and placing her in an ever-tightening Gordian knot.
By trusting my therapeutic authority, a focal theme emerged. When this patient expressed negative emotions, people could not tolerate them and emotionally and physically abandoned her. This pattern was consistent with her emerging friendships — others were not interested in hanging out with her despite her charm and intelligence — and extended to her early family experience, in which her parents subjected her to the silent treatment for days whenever her emotions ran too hot. Taken together, the patient internalized a message that her emotions were problematic and disruptive and that they must be put aside and suppressed. In other words, they became “not-me” and funneled into the dissociative symptom of cutting.
Until I was able to home in on a focal theme, I, like the therapists before me, was part of the problem, imagining in my countertransference that it was the patient who had the major issue. Internally, I underestimated how much my feelings were part of an enactment, containing only a small piece of the story. Initially, I was bracing myself for difficult work, assuming that the student had a great deal of pathology and would make little movement. In a way, I was reenacting the dynamic of the student’s relational backdrop, finding her issues disruptive to my sense of authority just like her parents and her prior therapists had — “it is not me, it is her.” By maintaining a therapeutically present stance, I was able to observe this crucial dynamic and incorporate it into a new understanding and relationship with the client.
Therapeutic authority led me to a focal theme that helped me see that it was totally understandable for her to shy away from sharing her intense feelings and need to hide and express them in her not-so-secret ritual of cutting. She was protecting both myself and herself from “not-me” and letting the world know, with what seemed to be twisted pride, that cutting was her right and a very valuable part of her emotional life. Looking back on that detail now, it was very prescient in the way it encapsulated her attempt to express and independently resolve her bind.
Reading and Tracking Changes
Guided by a mindful application of therapeutic presence and a discriminating use of therapeutic authority, the student went through the kind of musical sequence referenced above. Initially, having a therapist who was able to respect and receive the fullness of her experience without mistreating or abandoning her by becoming critical or explosive or falling apart was a tremendous step toward a new relational experience. The recognition that her focal theme was understandable and heard enabled her to begin to speak of it without the kind of shame and dissociation that often accompanies a “not-me” experience. It also enabled her to begin to trust and hope again.
She became inwardly and outwardly relaxed so that she could begin to examine the many facets of her current and past experience and thus begin the riffing that is essential to the jazz improvisation that is therapy. In short, she began to find and develop her own voice as a patient!
The patient could view her behaviors as more comprehensible and expressive of the hidden conflicts she had been harboring and that had been left unformulated and disconnected. This expanding sense of self-compassion became an important antidote to her cutting behavior and provided an alternative avenue for exploring and containing her emotional experience. Interpersonally, she became less defensive and fearful of others abandoning her, having had a transformative set of experiences in which she felt the consistent presence of a reliable other. She began to show her pain not only in her words but in the artwork, she did as a painter.
When a poetic turn or musical theme has been established, shifts can immediately be seen in the patient and felt in the relationship. These can occur simply in the change of posture (often, a straightening of the back and sitting up in one’s chair), a richer tone of voice, a feeling of newfound connection and space in the therapeutic relationship, or in the spontaneity and flow of narrative or images that emerge in the therapeutic interplay
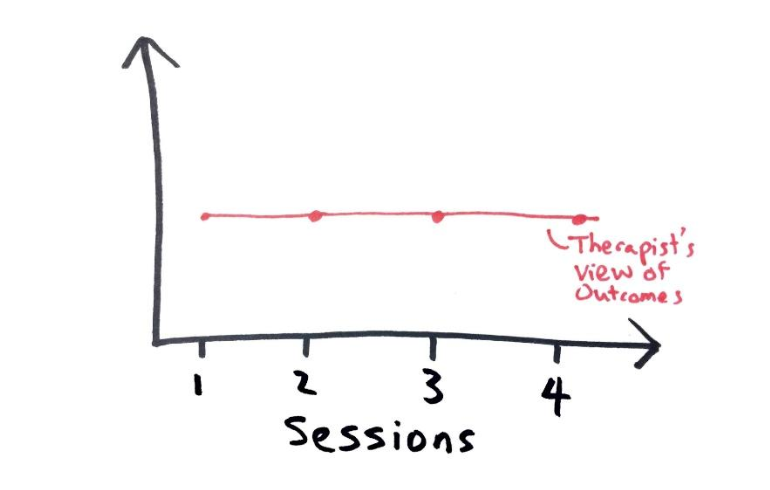
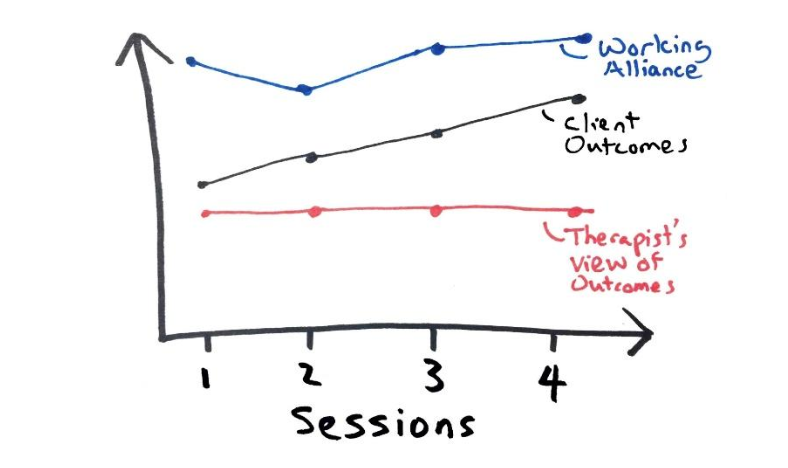
In the first session, trust was developed as the student began to see me as a figure who could understand and appreciate the depth of her pain and recognize the myriad ways in which she had been misjudged and pigeonholed by her family, friends and, most notably, other therapists. We also developed a focal theme centering on how this rejection led her to suppress and negate her important and precious feelings. Taken together, I believe that these turns led to decreased scores in hostility and emotional distress, each indicative of the fact that she was feeling more trusting, less defensive, and relieved at being able to begin to experience her emotions more directly.
These scores continued to remain significantly lower than baseline for the next few sessions, whereupon we worked on developing ways of shifting patterns in her relationships with friends and family. At around session five, the student’s depression scores started to decrease as she began to feel greater self-efficacy and agency in being able to affect change in her life inside and outside of the therapy space. Simultaneously, her levels of anxiety followed suit as they made a statistically significant drop from baseline in our final session of the semester. Our work together concretized the notion of making a more poetic and musical line in our therapeutic work, and the importance of drawing on artistic metaphors to inform treatment and expand both the therapist’s and the patient’s voice in that process.
A New Slant on Working Dynamically
We are very accustomed as clinicians to thinking vertically, troubling ourselves over quick diagnoses and assessments, especially given the limited time we often have. At some points, this may take away from focusing horizontally on the musical line and the movement of the intervention. In music, in order to play or sing a melody successfully, one needs to be as attentive to the horizontal motion of the notes carrying a melodic line forward as to the vertical axis of hitting the note itself.
In clinical practice, one can analogize the horizontal forward motion to the momentum of an intervention, the movement toward a new relational experience. The vertical playing of the note is the clinical equivalent of ensuring you understand the patient’s experience correctly and getting a proper diagnostic read. This horizontal motion is informed by therapeutic presence just as, conversely, the vertical movement is guided by therapeutic authority. Both are essential, and they need to be worked in concert to turn notes into music.
This musical way of approaching relational work helps us to be more efficient, fluid, and creative, focusing simultaneously on how to skillfully assess and intervene in our fast-paced culture. Moreover, it enables us to carry the themes of the patient’s past into new orchestrations and harmonizations in the present, providing a model for continued transformative possibilities in the future. Through this process, patients internalize working creatively with their own themes and then take us into new melodic and harmonic territory, stimulating further treatment progress and development. Taken together, this fosters a positive feedback loop in the creative matrix between patient and therapist, and from this synergy, transformative changes quickly follow. This is precisely what a well-tuned therapeutic voice does for the clinician and their client.
References
Cornfeld, F. D. (1965). Collected poems. Cresset Press.
Questions for Thought and Discussion
Who inspired you to find your voice?
What are some of the unique attributes of your therapeutic voice?
Which of your clients helped you to find your therapeutic voice?
In what ways do you compare psychotherapy to an art?






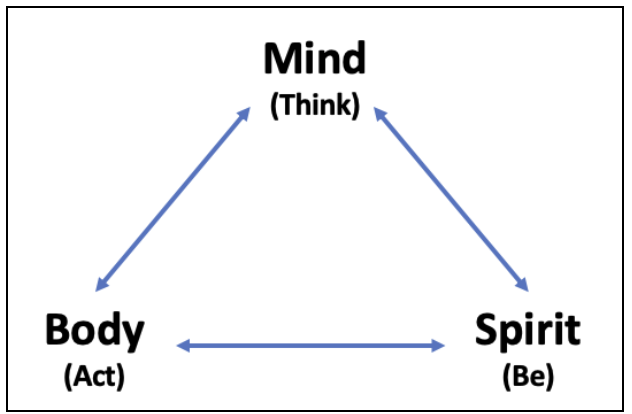 When I’m working with clients I often ask myself which of these paths might be most helpful to them at this point in their treatment.
When I’m working with clients I often ask myself which of these paths might be most helpful to them at this point in their treatment. We also worked toward taking care of tasks around the house that he’d been putting off and on building positive interactions with others since his relationships had suffered. Given his health challenges, we worked on ways to improve his sleep and eat more healthfully.
We also worked toward taking care of tasks around the house that he’d been putting off and on building positive interactions with others since his relationships had suffered. Given his health challenges, we worked on ways to improve his sleep and eat more healthfully.
