The Chicken Lady
When my now almost 30-year-old son and his brother were in elementary school, I took on a new role—the Chicken Lady. I didn’t intend to achieve that title, but it is one I hope I always remember because it symbolizes a pivotal moment in my time as a mother and a therapist. May we all have our own Chicken Lady experiences.

The Chicken Lady was born soon after I realized my children were speaking a language I didn’t understand in the backseat of the car on the way home from school. They were having a very in-depth conversation about a game they had recently started to play—RuneScape, which is classified as an MMORPG (Massively Multiplayer Online Role-Playing Game). It is essentially an expansive fantasy world where players can engage in interactions, quests, combat, and skill-building activities.
RuneScape emphasizes problem-solving and social interaction within a richly detailed environment. Typically, we would all chat together on the way home from school, discussing things that had happened during the day, what we would be doing over the weekend, and other such family-type things. When I began noticing that the conversations had shifted and I no longer understood the content, I felt a bit of sadness. To be clear, I am quite aware that kids will have their own interests and conversations. Individuation is an important developmental process.
In that moment, I thought about whether or not I would just leave this to them as their brotherly bond. I asked them questions about the game and one of them said, “You should just play it, mom.” And so, I did. This was the birth of my exploration into discovering the therapeutic value within all things digital. I witnessed the connection, the interaction, the executive function engagement (and more) within the play for my children, and I knew there had to be value within my work as a therapist as well.
Artificial Intelligence: A Brief Overview
Artificial intelligence (AI) is a very broad field of computer science focused on creating systems capable of performing tasks that typically require human intelligence, such as learning, reasoning, organizing, problem-solving, and understanding language. The term is attributed to John McCarthy and the Dartmouth Summer Research Project in 1956. As an aside, many people disagree with the term “artificial intelligence,” as they feel it does not accurately describe what this tool and process is. It is unfortunate because the connotation of intelligence that can mimic human processes often diverts conversations in ways that can be distracting. Science fiction writer Ted Chiang offers Applied Statistics as a very viable alternative. I am inclined to agree with him and his proposal of the term.Generative AI
Generative AI refers to a type of artificial intelligence designed to create new content such as text, images, stories, and more—to generate content through programs such as ChatGPT. Unlike traditional AI systems that follow predetermined rules, generative AI uses complex algorithms, often based on neural networks, to learn patterns from large datasets. This allows it to generate original and unique outputs that can mimic creativity and problem-solving skills.
It can be used for numerous day-to-day administrative (letters, session notes, treatment plans) and training tasks (learning objectives, quiz questions, slide decks, presentations) to create personalized therapeutic content (images, storytelling) and a variety of interventions and exercises. By integrating generative AI into therapeutic practices, therapists can offer more tailored and personalized experiences for their clients. In this regard, I offer the following table.
| Aspect | Description | Therapeutic Application |
| AI Learning Process | AI learns from large datasets including therapy concepts, psychology texts, articles, and more | Reading and collating large volumes of data |
| Text Generation | AI creates written content for therapeutic use | Writing personalized stories about overcoming anxiety |
| Image Creation | AI produces images based on descriptions | Visualizing a client’s experience |
| Language Understanding | AI analyzes and interprets context in communication | Grasping underlying emotions in client responses |
| Customization for Therapy | Adapting AI for specific mental health applications | Training on therapy techniques, adjusting vocabulary |
| Prompt Creation | Therapists and clients learn to craft effective questions for AI | Components and iterations inform the client’s conceptualizations |
| Continuous Improvement | AI refines outputs based on feedback over time | Learning over time provides improved responses |
| Multimodal Integration | Advanced AI systems work with text, images, and audio | Combining written responses with generated images |
| Ethical Considerations | Prioritizing client privacy and data protection | Ensuring the use incorporates confidentiality, secure data storage, and client protections |
Administrative Uses
AI provides a way to complete administrative tasks quickly in therapeutic practices, streamlining processes such as letter writing, case notes, treatment planning, and business analyses. For instance, AI-powered tools can draft and format professional letters, saving therapists valuable time while ensuring consistency and accuracy, or even help finding a synonym as I have done in this paper from time to time using ChatGPT. APA has even addressed how to cite the use of ChatGPT.
AI can transcribe session case notes, summarize key points, and organize information, allowing therapists to focus more on their clients and less on paperwork. This can also assist in treatment planning, creating templates and formatting documents as desired. Additionally, AI can assist in creating personalized, evidence-based, formatted plans by analyzing sanitized client aspects and suggesting potential interventions.
For therapists who provide trainings, AI can assist in the creation of required proposal content. If the trainer inputs a description of the training, the slide deck, or any other details, AI can generate elements such as training descriptions of specific lengths, trainer bios, learning objectives, quiz questions, and more. By providing the desired format (APA, multiple choice, true/false), prompts can guide AI to provide the information in ways that will minimize necessary alterations. All material should be evaluated and edited for accuracy. This is an area where the therapist’s expertise is critical to alter, amend, and/or add information. AI is here to format and collate information for the user, not to replace the therapist’s experience, expertise, or knowledge.
The Many Uses of AI in Therapy
Generative AI is transforming therapeutic practices by enabling the creation of personalized and vivid representations of a client’s experiences, narratives, hopes, dreams, fears, and visions. Generative AI can turn descriptive narratives (prompts) into detailed creations, providing a tangible representation of a client’s inner world. These aids are incredibly beneficial in therapy, helping clients articulate and explore complex emotions and thoughts that might be difficult to express verbally. By depicting their personalized experiences, clients can gain new insights and perspectives, facilitating deeper self-understanding and emotional processing.Images
Visual representations can both represent and communicate important components of a client’s life. AI image generation allows for the creation of personalized images based on descriptive prompts provided by the client or therapist. These images can depict complex emotions, significant life events, or abstract concepts that might be difficult to express verbally. For instance, a client might struggle to articulate feelings of isolation, but an AI-generated image can visually convey their personalized essence of this experience.
By providing a tangible representation of a client’s inner world, these images serve as powerful therapeutic tools. They facilitate deeper emotional exploration and understanding, enabling clients to gain new insights and perspectives. This visual aid not only enhances the therapeutic process but also empowers clients by giving them a new medium to express and process their emotions.
Stories
AI can create powerful therapeutic stories; it can craft personalized narratives based on a client’s experiences, dreams, or visions, creating rich and immersive stories that resonate deeply. These AI-generated stories can serve as powerful therapeutic tools, allowing clients to see their personalized situations from different angles, have a more objective view of representation, identify patterns in their behavior, and/or explore alternative outcomes. Narrating their experiences through AI-generated stories helps clients externalize and reframe their thoughts, leading to potentially greater clarity and emotional relief.
Interventions
Generative AI can be invaluable in discovering interventions tailored to individual clients. By analyzing a client’s unique experiences and responses, AI can suggest personalized therapeutic strategies and interventions. These AI-driven recommendations might include specific therapeutic exercises, coping mechanisms, or behavioral techniques that align with the client’s needs and preferences and the therapist’s theoretical foundation. This tailored approach ensures interventions are highly relevant, enhancing the overall therapeutic experience and outcome. Integrating generative AI into therapy not only personalizes the treatment process but also empowers clients by providing them with tools and insights uniquely suited to their personal journey.
Prompt Creation with AI
Creating effective prompts is arguably the most crucial aspect of integrating generative AI into therapeutic practices, particularly when exploring a client’s experiences, emotions, self-concept, identification, and representation. In the context of generative AI, a prompt is a carefully crafted input or question that guides the AI to produce relevant and meaningful output/responses. These prompts serve as catalysts for AI to generate content that mirrors the client’s inner world, whether through prompt creation, image generation, or narratives.A prompt can capture the essence of a client’s priorities, experiences, perceptions, thoughts, and feelings. Depending on the client and the therapeutic needs, the client or the therapist could create the initial prompt with iterations and changes guided by the client. Prompts act as powerful projective tools, revealing underlying therapeutic material. As the process unfolds, subsequent iterations allow for deeper understanding for the client and therapist. By refining the initial prompt to more accurately represent their internal landscape, clients engage in a valuable process of self-discovery and expression.
The iterative nature of prompt creation significantly enhances its therapeutic value. Each refinement can unveil new facets of a client’s self-representation, offering a fluid, dynamic, and evolving view of their inner world. As clients fine-tune their prompts, they embark on a journey of self-reflection, identifying and articulating aspects of their experiences that may have previously been unconscious or difficult to express. This process not only helps clients gain clarity but also allows therapists to track changes in the client’s self-perception and emotional state over time. By engaging with the AI-generated output—accepting, modifying, or rejecting it—clients further refine their self-understanding, benefiting both themselves and the therapeutic process.
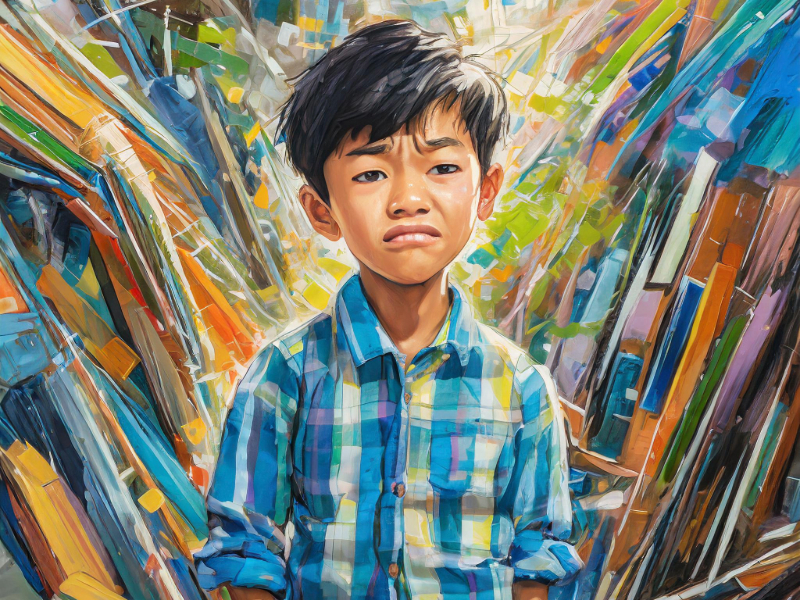
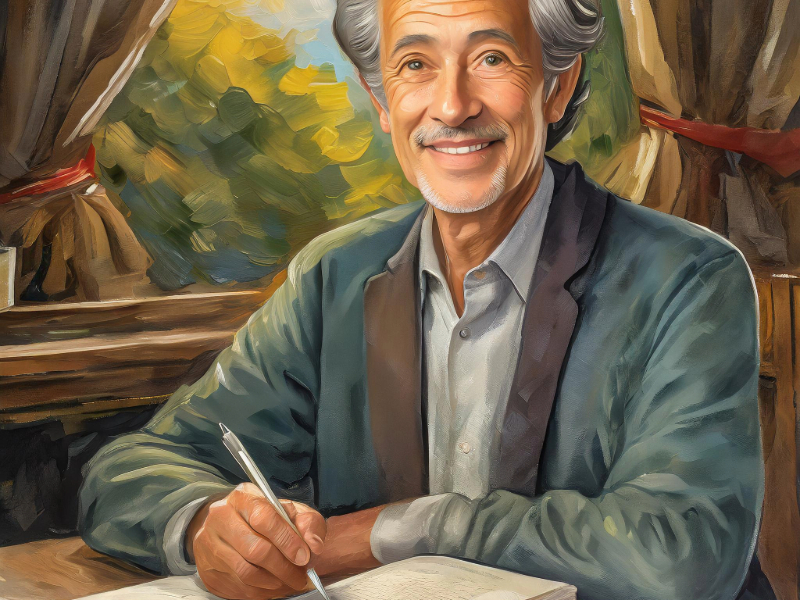
The therapist or client, or a combination of both, can lead the prompt generation process. For example, to help a client visualize a calming environment, a therapist may ask the client to “describe a place that feels safe.” This can include colors, items, people, animals, weather, and many other aspects. A client-driven image may include a request for something which depicts “a sad little boy with brown hair, brown skin, and brown eyes who is all alone in a storm.” Aspects which do not fit the criteria can then be changed through iterations, thereby revealing the client’s experience or desired depiction.
Prompt creation can serve as a projective exercise along with the desired creation. Each version of the creation, whether initial or refined, holds valuable insights. The evolving nature of prompts encourages ongoing dialogue between client and therapist, fostering a collaborative and exploratory therapeutic environment. When used skillfully and ethically, it can significantly enhance the therapeutic process, providing both clients and therapists with tools to advance the treatment plan forward.
The Ethics of Using AI in Therapy
The integration of generative AI in therapy presents significant ethical considerations, particularly regarding the protection of personal health information (PHI) and maintaining client confidentiality. Therapists must ensure that any data input into AI systems omits identifiable information as a safeguard of a clients’ privacy. This involves adhering to strict guidelines for data anonymization and being vigilant about the types of information shared with AI tools. Ensuring that all generated content complies with privacy regulations, such as HIPAA in the United States or GDPR in the United Kingdom, is essential to maintaining trust and ethical standards in therapeutic practice.As mentioned earlier, of key importance is the therapist’s expertise, experience, and training. While AI can provide valuable insights and tools, the therapist must have the final say in what is included and presented to the AI tool, and the decision regarding what type of output is generated within the therapeutic interaction. Therapists need to explore programs in advance and critically evaluate AI-generating programs, ensuring they align with therapeutic goals. This requires an understanding of both the technology and the therapeutic context, emphasizing the importance of ongoing education and supervision regarding the use of AI applications within therapy.
Case Example
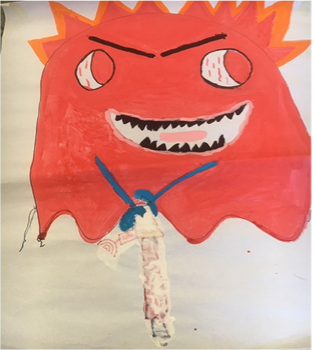
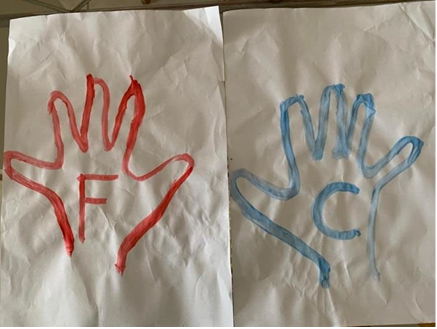
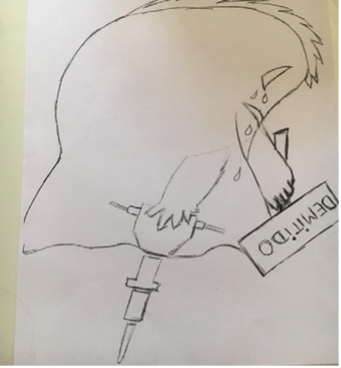
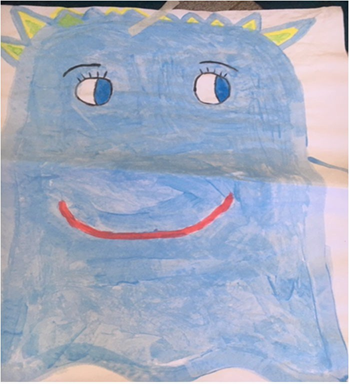
Emily is a 16-year-old transgender girl who presented for play therapy treatment during the transitional process of altering her gender identification and representation. She utilized generative AI to explore and articulate her experiences through image and story generation. Emily was assigned male at birth but discovered her identification as female. Among other approaches and interventions, her therapeutic process was enriched by the use of generative AI. She was able to visualize and narrate her journey of self-discovery, family acceptance, and social representation.Emily began her therapeutic gen AI journey by creating representative therapeutic images. She crafted complex prompts and many iterations that helped her create images which depicted her true identity as a female. Despite being born with male anatomy, these images allowed Emily to see herself in a way that felt authentic and congruent with her internal sense of self. The visual representations were a powerful tool in helping her recognize and affirm her identity, providing a sense of validation and clarity.

(Created with Photoleap, numerous prompt iterations -representations of Emily’s Work)
Therapeutic Outcomes
Through the use of image and story generation, Emily achieved several therapeutic outcomes:
1. Self-Representation: She was able to see a visual representation of herself that was congruent and customized to her experience.
2. Narrative Creation: Emily created a narrative that represented her journey, helping her process and make sense of her experiences.
3. Sharing with Others: She produced content that could be shared with others, both known and unknown, fostering understanding and support.
4. Prompt Iteration: Emily learned to determine the important components of her experience and represent them accurately through prompt creation and iterations.
A Beginner’s Guide to Generative Artificial Intelligence
Generative AI is a type of artificial intelligence that creates new content, like text and images, based on patterns it has learned from data. Unlike traditional AI, which follows set rules, generative AI uses complex methods to generate original outputs.Key Concepts of Generative AI:
1. Neural Networks:
- Think of neural networks as layers of connected “nodes” that process data, similar to how our brain works.
- They help the AI learn patterns in data, enabling it to create new content.
2. Training Process:
- AI learns from large amounts of data, such as texts and images.
- AI goes through the data multiple times, adjusting its internal settings to improve accuracy.
3. Generative AI in Action:
- Text Generation: AI models like GPT can write coherent text based on a given prompt. They are used in chatbots and content creation.
- Image Generation: AI tools can create images from descriptions, helping visualize concepts.
4. Applications in Therapy:
- AI can create personalized narrative content, like personalized storytelling.
- AI-generated images can help clients visualize their emotions and experiences.
Important Considerations:
5. Data Quality: The AI’s performance depends on the quality of the data it learns from.
6. Privacy: It’s crucial to keep client information private and secure.
7. Understanding Limitations: While powerful, these AI models have limitations and can sometimes produce biased and incorrect results.
Concluding Thoughts
Integrating generative AI into Digital Play Therapy™ marks a significant evolution in the field of mental health care. Through blending advanced technology with psychotherapeutic expertise, therapists can enhance their practice in multiple ways—from creating personalized therapeutic content to streamlining administrative tasks and discovering tailored interventions that resonate with each client’s unique experiences.
Just as I embraced the world of Rune Scape to connect with my children, therapists today can embrace digital tools, including generative AI, to form deeper connections with their clients. This technology offers unparalleled opportunities for creating vivid visual representations, crafting personalized narratives, and developing customized therapeutic strategies that cater to individual needs.
However, the integration of AI into therapy must be approached with careful consideration of ethical responsibilities. Ensuring client confidentiality, maintaining rigorous training standards, and critically evaluating AI-generative programs are essential practices that uphold the integrity of therapeutic work. Therapists must balance innovation with ethical responsibility to protect clients' privacy.
Thoughtful and ethical use of AI can allow therapists to enhance their practices by offering clients more options for engaging, insightful, and effective therapeutic experiences. The future of therapy is bright with the possibilities that generative AI brings. As we continue to learn and adapt, we can utilize these technologies to transform the therapeutic process in profoundly positive ways.