“There’s a boy, there’s a kid always living in my heart every time the adult shivers he comes and gives me his hand.” Brant and Nascimento [1]
My childhood has been a never-ending playground of theoretical and practical knowledge that has influenced my own evolution as a therapist working with children. In my work with children, I bring my own valuable child-within who leads me through the paths and crossroads of therapeutic work and inspires my imagination and curiosity toward a world to be discovered. Favored by being born into a family where other children arrived year after year, older siblings like me were taught to take care of the younger ones. I was privileged to be raised in a generation where neighborhoods were populated with children and playing in open spaces was imperative. Thus, in my consultations, echoing the lines of Brazilian composer and musician mentioned above, there is a child always living in my heart.
From this particular cultural heritage, I assumed positions that today I consider foundational for my personal relationships, and fundamental for my clinical practice. I understand that the therapeutic relationship with children requires letting oneself be carried away by playful and creative coexistence, and the belief in a collaborative relationship that transforms unhappy ways of living.
This article was produced because I felt invited to share a reflection on everyday clinical practice, understanding it as a written dialogue between me, the author, and other authors or readers. It involves the work I did with a family consisting of parents and two children ages eight and four. The consultations were mostly made involving the mother and her eldest son, whose main issue was the indomitable spirit that appeared whenever he was contradicted by her, with an abundant flow of anger, accusations, and dissatisfactions arising on his part and paralyzing her. These are therapeutic conversations that took place during the year 2020 and were crossed by the COVID-19 pandemic, which brings as a challenge the development of resources to maintain the therapeutic process.
In the dialogue with the reader, I intend to report fragments of the practice, seeking to give visibility to: 1) externalizing conversations as a ludic dialogical resource and promoter of preferable changes, 2) the production of therapeutic documents in the format of therapeutic chronicles (1, 2), a useful resource for pointing out remarkable moments in the participants’ reauthoring process, and 3) to the share of moments in which the use of online technology helped the co-construction of generative therapeutic relationships, making it possible to move forward in the conversational process.
Chatting with Some Textual Friends Before Entering the Therapy Room
Michael White (3), despite the expressive systematization capacity of his work as a whole, privileged the developments of his practice so that the spirit of narrative therapy could be expanded, without letting it be tied down by any preponderant discourse of this or that therapeutic school. David Epston, echoing this plurality of meanings in narrative therapy, points out both the irreverence, improvisation, and imagination present at the center of everyday life and the indignation with the injustice that generates human suffering (4). Thus,
narrative therapy actively questions the individual centralization of human problems and invites one to think about their insertion into the dominant social discourses that configure people’s lives.
As a therapeutic stance, this questioning promotes an egalitarian relationship between therapist and client and denies norms that subject people to standards on how they should be, feel, and act. Such a decentered position of the therapist facilitates a joint construction of choices that clients wish to assume about their problems and difficulties, based on the values and beliefs that guide their lives. Thus, change is built from new shared meanings toward the dissolution of the problem (5).
Narrative therapy discusses the deconstruction of the therapist’s power from a Foucauldian perspective that emphasizes power not as an institutional implementation from the top-down, but as one that develops and refines itself at the local level of culture (6). In other words, people are products and producers of relationships, concepts, and dogmas that shape dominant and socially constructed cultural discourses. Thus, in the therapeutic encounter, we are faced with problem stories that are saturated by culturally-sanctioned master narratives, which objectify people and describe them as problematic, paralyzed, and incompetent in promoting change.
To face the dominant stories that produce this deficit and limited identity construction, the externalization of the problem — later renamed externalizing conversations — was an ethical and creative response developed by Michael White (3,6,7) to counter the power of uniform descriptions about people, which engulfs all the uniqueness that each individual has in facing their difficulties. Such conversations, as a dialogical resource, invite participants to understand that the problem is the problem and not the person; an approach that encourages people to question the oppression that problems acquire over them, as well as to weave the reauthoring of their lives. Michael White says:
There is a sense in which I regard the practice of externalizing to be a faithful friend. Over many years, this practice has assisted me to find ways forward with people who are in situations that were considered hopeless. In these situations, externalizing conversations have opened many possibilities for people to redefine their identities, to experience their lives anew, and to pursue what is precious to them.
This fascinating spirit that rests on what is unique in each person and is so present in working with children is reflected in the enthusiasm of another young client: “I said to my father: ‘There must be some magic here! That cry that I used for everything disappeared!’”
With the inspiration of “as if it were magic,” I will present below the report of the family care on which this article was based. The meetings were mostly attended by the mother (Aurora) and her eldest son (Daniel) since the difficulties described brought many misunderstandings and a feeling of hopelessness in the relationship between them. Since problems organize the system, Leo, the youngest brother, was included when conflicts between children intensified with the social isolation imposed by the pandemic; the father could participate in only a few sessions, when we managed to schedule appointments after his work shift. In these meetings, where the whole family got together, playing freely was the main objective (8).
A Cry for Help
Even in the first days of the January 2020 holidays, Aurora, the young mother of Daniel (eight years old) and Leo (four years old), was very distressed at not achieving a balanced relationship with her eldest son, who “throws himself at the television” and does not commit to his obligations, from taking care of personal hygiene to school obligations during class time. Born at 7 months of pregnancy, he was assessed during the literacy period and received a diagnosis of Attention-Deficit Disorder (ADD), in addition to living with an uncomfortable dysgraphia and psychomotor immaturity, which forced his mother to follow up on school tasks, correct spelling, and “correct the ugly handwriting.” Always complaining, he got irritated when his mother pressured him: he screamed, cried, and accused her of being a bad mother. It left her “out of her mind,” since she did the best she could. In those moments, anger also dominated her, from which words emerged that she would never have used if she could think before speaking. She therefore felt very guilty and convinced herself that she really wasn’t a good mother.
Aurora was also concerned about her younger son. Like his older brother, he was born prematurely, but perinatal complications and the effects of early birth were more invasive in his development. The parents began to protect him, offering him little encouragement in the autonomy of daily life activities: “He is our baby,” “required a lot of care,” “was always weak,” and “cries to get everything he wants and I end up giving in so as not to get angry anymore,” said Aurora. A kind of vicious circle was established, where Daniel’s defiant attitudes and Leo’s insistent crying resulted in a joint explosion of irritability. In this way, by giving in to her children’s demands, Aurora obtained a moment of peace: “I end up giving them what they ask to put an end to the complaints,” to soon after, be taken by guilt and the uncomfortable feeling of impotence in the face of the conflicts.
The family had moved to the city of the maternal grandparents two years before, in the hopes of receiving family support for the care and treatment of their children. They left behind schools, relationships, friendships, leisure, and professional stability. They faced professional and financial obstacles and the expected help from their family members did not materialize. The couple underwent a reorganization of their responsibilities as family providers, with the children’s father expanding his professional activities, while Aurora saw hers reduced due to the care and education of her children. Thus began a lasting period of frustration, overwhelm, and exhaustion.
“Hello, May I Come In?”: Expanding the Meaning of the Problem
Aurora and Daniel attended the first meeting. Daniel was a silent and observant boy apparently uninterested in participating in the conversation that concerned his failures in everyday life. Aurora spoke about all her disappointments with her son, such as: watching too much television, complaining about everything although she was always helping him, lacking autonomy for schoolwork, avoiding physical activities, and being uncooperative and disobedient to his parents’ expectations. His greatest difficulty, however, concerned the inability to control himself before exploding into fits of rage when contradicted. Uncomfortable, Daniel silent and sad, slowly walked away and disappeared from the room. Another environment was more interesting to him: the playroom.
I invited the mother to accompany him and, looking for a way to involve him in the issue that brought them to the consultation, I said that many children suffer from all sorts of problems, and that, as if that were not enough, these problems also interfere with the lives of their families. Curious to know the face of the problem, I asked if we could take a picture of it; problems that haunt children’s lives are invisible and we can only get to know them by drawing them. Continuing, I said that a camera has not yet been invented to register the existence of these beings that disturb people so much. The mother looked open and curious; Daniel looked incredulous at what he had just heard. Aurora took the initiative and soon the two of them found themselves sitting on the floor, dealing with paper, brushes, paint, and enthusiasm.
While planning what could be drawn, a different conversation took place. New vocabularies sprouted from a much more collaborative mother-son relationship: “Is it a monster or a ghost? It’s quite big, so it needs a larger paper. It has a skirt, and many teeth in the mouth; the hair is spiked.” Daniel started to see the image of the problem: “Mom, the monster will be red, because red is the color of anger.” The boy, encouraged by the change of direction of the conversation, busied himself in coloring with care and the mother patiently accompanied him in the dance of the brushes. By photographing with paints and brushstrokes, the problem takes on form: “Wow! It’s nice! Mom, you look mean!”
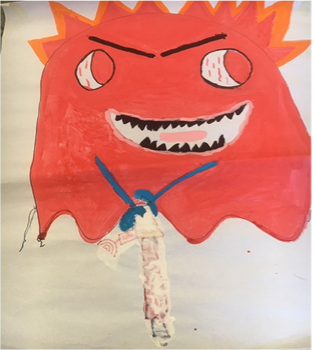 Ghost of Fury
Ghost of Fury
Satisfied with the reproduction, Daniel says: “It is a giant of Fury that torments a lot, attacks the head, and keeps hitting it.” The part of the conversation below illustrates the dialogue that is being woven around the externalized problem (the acronyms T, D, and A, refer respectively to Therapist, Daniel, and Aurora):
T: I think he has a jackhammer in his hands and drills holes in your head to get in! (I paint a tool in the hands of the giant). Could we come up with something to let you know when he’s turning on the jackhammer? (I paint a radar that says “No,” when it notices that the giant is approaching).
D: No… it crosses your mind… It’s a ghost.
T: Oh! We are getting to know him better! He looked like a giant, but he’s a ghost!
D: Yeah, he doesn’t drill holes; it goes through the head (erases jackhammer drawing with white paint).
I understand that this attitude of Daniel concerns his authorship, and he gradually builds on his relationship with the problem. It’s like he’s saying, “Hey! This is my problem!” There is a significant change in how he relates to exploring the difficulties that brought him to therapy.
The separation between the person’s identity and that of the problem does not exempt them from facing the damage that this has brought to their lives. According to Michael White, it enables them to assume this responsibility, and, in this way, they are encouraged to establish a more clearly defined relationship, in which a range of alternative possibilities becomes possible. And continuing…
T: And does he take advantage of some “little windows” to get inside your head?
A: I think it’s when he gets jealous of his brother and when we go against him.
An alternative way of talking about the difficulties that permeate family relationships is under construction without, however, pointing out the child’s deficits, and blaming him. Externalizing conversations, by objectifying the problem, offers an antidote to internal and essential understandings of an individual.
Building an Identity for the Problem
The problem, now named Ghost of Fury, is gradually discovered through a curious investigation where I learn from the clients about their experience. The Ghost of Fury is 1,000 years old and lives in every child’s house for one year. It arrived when the family moved from the city where they lived two years ago, leaving the loving paternal grandparents. He feeds on people’s anger and his favorite food is “rage burger.” He lives in hell and other evil ghosts also live there.
Upon hearing Daniel’s vibrant description, Aurora reported that the parents and children lost their friends. The children separated from their schoolmates, from the playground in the old house, and from the paternal grandparents’ beach house. She says: “Daniel always says it was my fault we moved here. He doesn't like it here.”
D: Yeah, we had to come here because she got a job here…(
notices the mother’s tears) Mom, are you crying??!!!!
T: I think you were all very sad to have moved to another city. Nothing happened as you expected…
A: He says I'm not a good mother, I feel very guilty. I do everything for them, I can hardly even work…
T: Yeah… one of these evil ghosts’ tricks is to make mothers feel guilty. They disrupt the whole family’s life.
D: Not my father’s life! He works and comes home late and just sits on the couch watching TV, right mom? (
Aurora laughs).
Looking for the influence that the problem has on the life of Daniel and his family, I highlight the following excerpt:
T: What does he want for your life?
D: That I become evil? He wants me to be mean!!! (
His eyes are wide open, pointed at his mother).
It is important to note here the change in the child’s expression that seems to reflect on the influence the problem has on his life and suddenly discovering his real purpose. And continuing:
T: And what does he want for your family?
D: He wants us to fight, stay in front of the TV alone, without talking to our mother, without playing… He doesn’t just disturb the family; he also goes to my (maternal) grandparents’ house. The most nervous is my grandfather. He drives my grandfather crazy.
D: Mom, grandpa needs to come here too!
Michael White says that this type of conversation, through influencing questions, compares to investigative journalism and its first objective is “to develop an exposition of the corruption associated with abuses of power and privileges,” imposed by the problem. Like investigative journalists, therapists are not involved in the domains of problem-solving or engaging in conflict, but, again referring to White, “Rather, their actions usually reflect a relatively ‘cool’ engagement.” In contrast, clients also assume an investigative reporter position, reflect on their experience, and contribute to exposing the character of the problem. They denounce its objectives, purposes, and activities.
This posture reveals the importance of the narrative therapist’s decentered position. It paves the way for the clients to identify and build other plans for their lives, what they value, and contradict the threatening voices of the problem. In other words, externalizing conversations offer a shared island of safety for people to engage in the reauthoring of their lives.
A Story About the Externalized Problem Inspired by the Idea of Poetic Documentation
For White and Epston, the written word is an ideal path for discoveries made during therapy which, like documents, can be evoked, read, and recreated. Written tradition, through “making visible,” highlights extraordinary events, giving prestige to an alternative narrative (9). Still, according to Campillo Rodriguez (1), writing as a therapeutic resource opens up many paths through which people can see themselves through the eyes of the other.
During clinical consultations, therapeutic poems build, in a special way, an opening to new stories, which play with the imagination and give clients the freedom to experience their own images, sensations, and new meanings.
Discussing the usefulness of therapeutic poems in her work, Sanni Paljakka (2) writes:
Due to their unusual form (the lack of requirement for the shiny completeness of sentences and ideas in prose text), these poems have opened up a unique way for me to play with ideas. Writing in poetry form allows me to pit the horrors and hauntings of a problem story against a confection of possible counter-story ideas with no regard to orderly sequencing of life experiences or the flow of a therapy conversation.
So, at the opening of the session following the revelation of the Ghost of Fury, I asked Daniel and his mother to sit down comfortably and listen to a text that I wanted to present to them (Although the authors point out that poetic documents should be written exclusively with the words expressed by the client, I took this therapeutic tool as an inspiration, adding a personal way of narrating, to what I preferred to name therapeutic chronicles.):
It was a problem and it was a gigantic
A giant that was so gigantic, it tormented everyone
It tormented the boy even more
The boy was a child
And he did the worst for the child Just for the kid, he had a jackhammer
He made little holes
In the boy’s head
When he was a child and the boy was a child
Clever
Thoughtful
Observer
And the boy had an artist mother
The child boy had an artist mother!!!
The smart boy and the artist mother took a picture of the giant
Click, Click, Click
Red he was
With funny hair and there was the jackhammer Making holes in the head
And making everyone nervous and quarrelsome and then… Sad
And found out the giant was all Rage Aha!!!
Now we know you!!!
And the smart boy and the artist mother didn’t notice…
The Giant of Rage, that was his name, was very intelligent
In a brush step, zas!!!
Changed to Ghost of Fury
What the hell!!!
Ghosts don't need little holes to get into the heads and families of smart boys and nice moms
Ghosts walk through walls
The smart boy figured out the trick. He found that the ghost goes through his head
And lo and behold! He knows many tricks to do bad things
He is 1,000 years old.
I recited the chronicle, dramatizing it in such a way that the emphasis fell on the resources and extraordinary events subjugated by the problem (the boy was a child; he was smart, thoughtful and observant; the child had an artist mother; the smart boy and the mother artist took a picture of the giant), as well as the perverse purposes fueled by the problem (the giant that especially affects the boy, who is a child; his evils are preferably directed at him; a very intelligent giant, who magically transforms into a ghost to cross heads).
As an externalizing conversation, listening to your experiences coming from another person, written in a poetic way, promotes a sense of legitimacy and centers authorship on the person. Afterward, Daniel said he liked it and thought it was funny: “He doesn’t even look that bad!” He still prefers to maintain his version of the problem as a ghost that enters his head without making small holes: “Hey tía, he doesn’t have a jackhammer.” Aurora was touched by the understanding that her son is “just a child” and that, due to so many turbulences in the family, her impatience could be harming him, in addition to expecting him to know how to renounce his place in the family in favor of his younger brother.
It was surprising to her to be perceived as an artist and she reported other craft skills, inherited from her mother. Daniel praised his maternal grandmother’s skills, attentive and creative, and discovered that his mother resembles her. The externalized problem, re-narrated, allowed the emergence of a narrative not subdued by the history of conflicts in the period between the meetings. Aurora says:
A: The giant isn’t showing up much there… he’s only showing up with strength when he’s with his brother. They fight, Leo gets in the way, and Daniel loses his temper (the words giant and ghost will alternate during the course of therapy, as meanings of an entity/problem separate from the child).
T: I think it’s the Giant of Fury’s tricks to keep taking advantage of the fights in your family.
A: He (Daniel) is better than me, calmer than me, he obeys when I speak.
Despite the influence of the problem having diminished in the family, this meeting addressed many conflicting moments between siblings and between mother and children. Daniel suggests painting the Giant/Ghost again. Very excited, he announces:
D: Now I’m going to do it! It will have two colors. Half angry and half calm.”
The new image of the problem in metamorphosis was made with four hands, and the child tried to reproduce with his own lines the first form almost entirely created by Aurora (the Giant of Fury). This was explored in its finest details within a loving and respectful dialogue, mostly coming from the child. Everyone looked proud at the end.
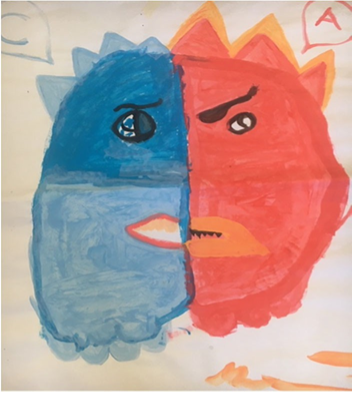
Ghost of Fury in Transformation
The letters C and A were added to signify the initials for Calm and Angry, English vocabulary learned by the boy at school. Descriptions and facts previously mitigated by the problem populate the conversations, allowing the child to be perceived through his resources (learns another language, likes to paint, collaborates with the mother). Immersed in a dialogical and horizontal relationship, instigated by conversations fueled by painting, I outlined Daniel’s hands on a blank piece of paper, with the letters F (Fury) and C (Calm) to be taken home. They could help them remember that when they manage to stay calm, the Giant weakens.
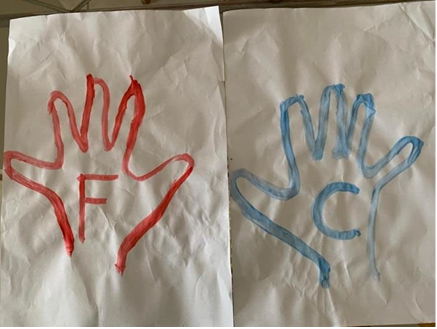
Drawings of Daniel’s Hands as signalers of emotions in the house
The session that followed this one focused on efforts to distinguish the influences of the Giant/Ghost in the family’s life and the family’s in the Giant's life. The rage attacks are less intense; frustrations are expressed with lamentations. Aurora says:
A: Daniel is more loving, more understanding, helping me to calm down faster. It was a lot of just complaining, now it’s like this, more smiling. Sometimes he is more patient with his brother.
D: I didn’t get angry with Leo crying. I say: ‘Caaaalm down, Leo’.
A: We put the Hands in the room. In a place where everyone can see.
T: If the house is calmer, how is the family?
A: I bought paints, they are painting.
T: It’s a family of artists!
At this time, they review the contributions of their maternal grandmother, skilled in manual arts. Daniel speaks proudly of his grandmother who draws house plans for engineers. Aurora has the opportunity to reframe her relationship with her parents, with whom she feels hurt by for not receiving the expected support: “My parents are very active, they have a life of their own…”
Daniel is attentive and praises his grandmother’s kindness but claims that his grandfather is very nervous: “The ghost must be living there now.” and continues… “Hey tía, I think next time the Giant of Fury will be all blue!”
From these conversations, another poetic document was presented to them at the next meeting.
It was a giant
Giant?
Not anymore
It wasn’t even a giant. It shrunk
And in its shrinking, OH! Would it also be changing color?
And the giant asked for help
Help! Somebody help me!
I’m shrinking and I’m not even red! Help!
And nobody listens
The artist mother and the smart boy continue their task of transforming him
Now the little giant is red and blue
Half bad, half good. Half angry, Half calm
The smart-mother and the artist-boy continue their work of painting the new little giant red and blue
The Giant of Fury is sneaking out
It no longer fits in that room. It no longer fits in those lives
At the door, already saying goodbye, he looks back and takes with him an image that bothers him. He sees the boy-artist calmly walking around the room, talking to his smart-mother, deciding together on the last brushstrokes.
The image has changed. And the Giant of Fury, sad, decides to leave in search of another place to live.
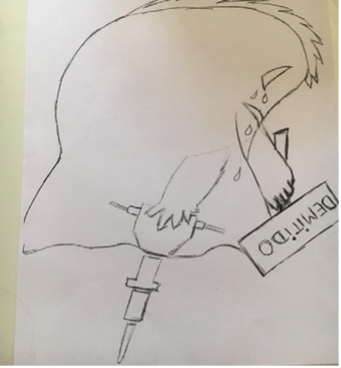
“The Fired Ghost of Fury,” Made by an Artist Upon my Request
When presented with the new image, this time taken by me, the mother laughs at the ghost and its “Fired” sign. Daniel says: “Poor guy,” and, “Mom, we’re firing him from home too!”
With a social constructionist sensibility, narrative therapy assumes that the self is relational. Within the plasticity of relationships, we build reciprocal identities, shaped by contextually-situated linguistic descriptions. Thus, Daniel’s interest and initiative, in a safe and inclusive environment, transform him into a boy-artist, now accompanied by a smart mother who, less confused by her feelings of incompetence and guilt, becomes someone who knows how to take action (welcoming, encouraging, believing, hoping). Therefore, the Giant who abandons that relationship is one of misunderstanding, impotence, and pain.
The self-confident artist-boy prepares to paint another ghost: “I do. It will be all blue. Blue is the color of calmness, right mom?”
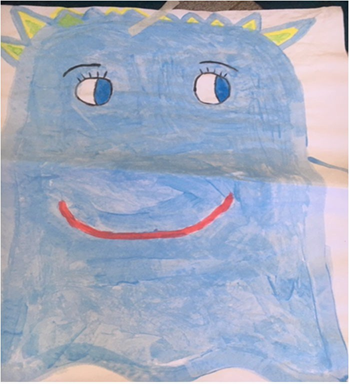
Ghost of Calmness
Since we were at that moment on the verge of social isolation due to COVID-19, we suspended face-to-face meetings and sought to build communication via WhatsApp, through messages and audio, since the video camera sessions proved to be unproductive for the participation of the children. Contacts were more frequently aimed at supporting Aurora’s concerns regarding Daniel’s growing lack of interest in online classes. Still, mother and son agreed that the Ghost of Fury was still diminishing. In this period of confinement, the interaction between the two children deteriorated, slipping easily into conflict. I suggested that Brother Leo be invited to participate in a face-to-face meeting, and we all committed to this meeting, respecting the health standards for disease prevention.
The dialogue below illustrates a remarkable moment from this meeting, where many disputes took place, with Daniel asking for his mother’s interference to calm down and hold his brother who “only gets in the way” an