Victor Yalom: Welcome Judy. I wanted to start out by saying how grateful I am that you’ve recently trusted psychotherapy.net to publish the vast video library you’ve created, containing over 100 expressive arts therapy titles. It’s truly an honor for us to be the caretaker of this unique and incredibly valuable library. So, thanks for that, and before we talk about the collection, I want to get some context. I understand that through some interviews you’ve given, that you were there when art therapy was just starting as a field of study and practice. I know there’s not just one art therapy, but to get us going, how would you define art therapy or art therapies? What does that really mean?
Judith Aron Rubin: People get caught up in trying to define it, but it’s simple in my mind. Art Therapy is using an art form, in my case, the visual arts, to help people through therapy. And yes, there are many variations; but in its essence, it’s art plus therapy.
The Therapeutic Value of Art
VY: Why introduce art in therapy?
JR: As it turns out, and I guess we all know that we don’t start out having words as infants, but we do start out having visual experiences. Other art forms like movement, drama, and music also depend on some of the other basic sensory inputs babies have. So, these are simply ways we learn early on of taking in information about the world and then expressing experience.
To not take advantage of these natural and inborn languages in trying to help people get better seems almost foolish. Cooing, babbling, dramatizing, pretending, and making marks seem universal in higher primates. When given art materials to make marks, chimpanzees and apes like to draw and paint. So, it’s a natural activity that can be used to help people — another avenue to reach people and to help them find out about themselves.
VY: Art Therapy is using an art form, in my case, the visual arts, to help people through therapy. It makes a lot of sense when you think of it that way because one of the things we’re always trying to do in therapy is to get people to explore new things and come to new understanding about themselves — although not necessarily to a non-verbal place. I know you were trained as an analyst and that in analysis, the clinician uses techniques like free association to help people discover new things about themselves by exploring their unconscious or preconscious. This sounds similar to your way of describing the use of art in therapy, although it’s probably more expansive.
JR: That’s one way of looking at the value in people expressing themselves freely like free associating with words. Free association and images is actually quite fun. And you can do it with mental images. You don’t have to draw or paint them. And in fact, there were a lot of psychologists in the 60s and 70s and 80s who were quite interested in mental imagery as a way of understanding, but also helping people.
VY: creating something visually, or moving or dramatizing, are all ways of cutting through those defenses. So, it’s tapping into these other ways of experiencing and seeing the world. How is that helpful to clients?
JR: Because they can get in touch with things that they are unable to articulate in words. It’s obvious with people who are not very verbal, or who are communicating to us through a second language, or who have hearing or expression problems. But it’s also very helpful with people who intellectualize, who use words defensively to cover up. They’re not aware that they’re doing that, but that happens. Creating something visually, or moving or dramatizing, are all ways of cutting through those defenses, allowing something to become part of someone’s awareness that they couldn’t otherwise access.
VY: There are two interesting points that I hear you making. One is that art therapy can be very helpful. It seems that it has historically been used quite a lot, and probably still is. I think non-art therapists think of art therapy being used more frequently with these populations who aren’t as verbal, and who may be in hospital settings with psychotic patients or others with other disabilities.
What I also hear you say is that it’s very helpful for people who intellectualize, which is a large percentage of the clients we see, especially higher-functioning ones. That can be a real limitation in therapy. People can talk about themselves; they can theorize and intellectualize about themselves; they can tell stories and come up with intellectual and rational explanations. But that doesn’t necessarily lead to anything happening therapeutically.
JR: Yeah, it’s interesting because using art in therapy seems to help people not only get to a kind of awareness or insight, but also to feelings that they aren’t aware of that are often evoked by using art material or seeing what they’ve created with the material. This can be incredibly powerful.
And the Children Shall Draw
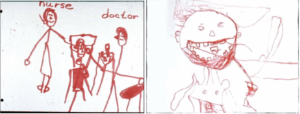
VY: I’ve just had a chance to look at a few of the videos in the vast library that you’ve created. One image that struck me was when you were working with a young girl who was non verbal. People thought that she was “retarded,” which was the term used at the time. She drew this incredible image of going to see the dentist. Do you remember that?
JR: I do. That was 1967 — three years before the American Art Therapy Association was formed. You’re right that it was in the beginning years, and that was exciting. Actually, it was fun. I feel lucky to have entered the field at a time when it was essentially unformed. It was about ideas and passionate people. But there hadn’t been any kind of intellectual framework developed yet.
VY: I feel lucky to have entered the field at a time when it was essentially unformed. It was about ideas and passionate people. This is perhaps an example of the power of art that I can refer to one image someone created in 1967, and it can immediately evoke that same image in your mind.
JR: I not only remember the image, I remember the little girl who came into the art room in her wheelchair. I remember watching her create it and thinking, “God, this kid is not only not retarded, she’s saying something that needs to be expressed.”
VY: But she’s saying it through a picture.
JR: Yes. We were assessing children in a place then called the Home for Crippled Children, meaning it was all children with disabilities, some of whom were residents and some of whom came during the day. They had about 200 kids and had invited me to start a pilot art program because they had never offered art for the children. I met with the coordinators who presented me with a list of 10 eligible children. I remember saying, “only 10 out of all these children?!”
They were so anxious about what these kids could or could not do, so they picked only the 10 highest functioning children with the most mobility and fine motor skills. I asked if it would be alright if we assessed everybody, which they agreed to. As a result of this assessment and this drawing, this little girl was moved back into the classroom that she had been taken out of.
VY: Many therapists may think, “I’m not artistic, so this isn’t for me.” Is that a common thing you find?
JR: Oh, sure. Many patients and adults too. Except for children. Most children don’t say that. But adolescents? Adults? Sure, but then you explain.
VY: That’s interesting that kids don’t say “I can’t draw, I can’t dance, I can’t sing.” It’s something they do naturally. And then what happens? How do they go from there to this idea that I can’t draw, I can’t dance, I can’t sing.
JR: It happens developmentally around puberty, where they become much more self-conscious in the general sense about the way they look, the way they move, the way they dress and how they draw. They become self-critical. It isn’t simply their artistic talent or lack of it, because until a certain age, most kids are un-self-consciously able to create.
There are little children of all ages who are blocked, who are unable to play. These children really need creative arts therapy because it’s a kind of play therapy. I think the creative arts therapists in their training, in their experience, are used to helping people who can’t create, to be able to create, if that makes any sense. It’s part of the job.
Bringing Art into the Room
VY: Let’s get into what art therapy is, and how you use these natural, innate abilities in a therapeutic context to help people. That’s a big question.
JR: It is a big question. With different age groups, you present it in a different way, so I’ll just stick to art therapy for the moment because that’s what I know best. But, as I said, older children, adolescents, and particularly adults are inhibited. You explain that this isn’t about being an artist.
In fact, artists are some of the hardest patients in art therapy because they’re so aware and self-conscious about their art, and they want to make it pretty, good, and attractive. But that’s not the purpose of art in therapy. The purpose essentially is to help people express and find themselves.
VY: Some of the people reading this interview may be art therapists or know something about art therapy, and want to hear from you as a renowned figure in the field. But many others are therapists who have had no exposure to art therapy, so I’m wondering how, if you’re not trained as an art therapist, can you still start incorporating some of this into your work.
JR: I believe you can. It’s an issue, a political issue within the field, because it’s been difficult for art therapists to be recognized as clinicians. But in actuality, the training is at least as rigorous, if not more so than the training that LMFT’s and social workers and other masters-level clinicians receive. I believe it’s at least as good as, if not better than, the training that mental health counselors get. And many people go on for PhD’s these days in art therapy or related fields like psychology, which actually is what I did my doctorate in. So, I’m licensed as a psychologist, although I don’t think of myself as primarily that.
There’s some anxiety about sharing techniques and activities with people who aren’t trained in the art form or who don’t know how to help people to use clay or the paint or whatever, and may not understand what they’re unleashing. The truth is that you can get to buried material that can be quite disruptive unless you know what you’re doing as a clinician or therapist. That’s the political aspect of helping others to use art. But I personally believe that everybody should be incorporating it. I wrote a book called, Artful Therapy for Non Art Therapists.
VY: I think giving people choices is one way to help them overcome some of the inhibitions around using art in therapy. Whether someone is trained as an art therapist or not, can you say a little bit about how to introduce some artistic activity, whether painting, clay, drawing, or whatever into the therapy?
JR: That’s a whole chapter in a book, and a bit hard to put into words. One way is to help it be a non-threatening activity, because a blank piece of paper is pretty threatening to most adults. What has worked for me is to give people choices, to have options. I’ll say something like, “You can use clay, or you can use chalk; or if you prefer to use markers or colored pencils, that’s fine. You can use a little piece of paper or a big piece of paper, whatever suits you.”
I think giving people choices is one way to help them overcome some of the inhibitions around using art in therapy. It’s about explaining to an adult or adolescent that this is a way of getting at stuff that we might not otherwise be able to get at by talking. Another way is to ask people what they remember about their dreams, because dreams contain many visual images, so in a sense, they are already thinking as an artist.
VY: So, you give people a choice by starting out with some of the materials in your office or encourage them to have some of these materials available if you’re working online with them. What kind of instructions do you then give them?
JR: These can range anywhere from open-ended to a starter. A starter is an easy and non-threatening way to begin because it doesn’t push the person in one direction or another. You can put a blot of paint on paper, fold it, and then ask the person what it reminds them of. People also like to doodle or make squiggles, so you can ask them to do that with their eyes closed and then look at it, and then turn it around as you ask them, “what does this remind you of?”
Each time, it’s like a Rorschach as you ask them what they see. You can get a lot of projective material from this very simple exercise. Then you can say, “OK, now take all the other colors and make it look like what you saw in it.” Because it starts with the scribble that doesn’t require people to think of making something realistic, they’re liberated.
VY: The idea is that you want to reduce the resistance people have to drawing, or to art in general. And whether it’s an inkblot or a squiggle, you’re priming the pump.
JR: Yes, because just starting with a line or a shape doesn’t give you much. But when people start to develop an image, they can begin to see something, like an image in the clouds. That’s another common experience that you can remind people of to let them know that they don’t have to be an artist to be artistic. Or you can give them clay to fiddle around with and then ask them similar questions to those you asked about the doodle, squiggle, or ink blot.
VY: I’m sorry to interrupt here, but this reminds me of the walk I just took with my 92-year-old father, who was looking up at clouds and seeing faces in them. In an earlier stage of his life, he was not a visual person — he was a very word-and-intellectual person. In that moment, I saw him opening up to a different world in that way, which perhaps is something that happens with the elderly. Just an aside!
JR: That’s fascinating because he’s not the first person I’ve heard that about. I think it’s uncommon that people who were mostly word people begin to pay attention to sounds, images, and the nonverbal when they get older.
VY: Getting back, you started describing the process of helping people go from a doodle to filling it in. From that point, how do you do more? How do you work with that therapeutically?
JR: Well, let me give you another kind of example of helping people get started, one that’s very valid, and a bit different from that other making-and-creating exercise. We used to have more magazines for selecting and cutting out pictures to paste into a collage. You certainly don’t have to be an artist to do that. You just find the images you like — or even just projectively looking at postcards or small reproductions of artwork and saying something like, “pick the one you like or the one you don’t like and let’s talk about that.” You can use art as a stimulus and find non-threatening ways of helping people to get started creating.
VY: How do you connect that with the therapeutic issue that someone comes in with like a relationship breakup, or if they’re feeling depressed, or not sleeping well. These are some of the bread-and-butter issues that therapists deal with. How do you relate to that?
JR: If it’s a grown-up, you have to listen to them first. You don’t throw the art at them right away unless they say, “I’ve come because I want art therapy,” which sometimes happens, right?
VY: there are many ways of hooking into what they’ve talked about and asking them to think of it visually. If you’re an art therapist, it’s more likely to happen.
JR: But if they’ve been in verbal therapy and they’ve hit a block and they hear somebody say, “Oh, you can past this in art therapy,” they might then ask you, “Can I do some artwork?” But most of the time, people want to tell you what’s troubling first. You know, you don’t even have to ask, why are you here? They tell you pretty fast while they’re here. And so, you listen to that and sometimes you can say, “could you make a picture about that?” or, “what color would that be?” or, “what shape would that be, that issue you’re talking about?” or, “if that person was a color or a shape, what would they be?”
In other words, there are many ways of hooking into what they’ve talked about and asking them to think of it visually. And then you might say, would you like to make some art to see if that would help us? When I had adults in private practice, I would give them a choice of working at the table or the easel, or while sitting looking at me, in which case I would give them a sketchbook and they would sketch. I didn’t have to look at what they were sketching.
Sometimes, they want you to see it and sometimes they don’t. There’s a million different ways and I think one of the advantages of being in different positional relationships is also interesting. It’s not something you do in therapy as often, although some people like August Aichhorn went for walks with his patients. Some people do, but mostly people are sitting looking at each other, and if you’re an analyst, they’re not looking at you. But anyway, in the creative arts, there’s much more flexibility about how you are in space with one another.
VY: Even though we may think of ourselves as progressive, liberal, or open-minded, therapists like everyone else are creatures of habit who get locked into specific ways of interacting with their clients. Analysts traditionally didn’t look at their clients, and that progressed to primarily weekly, face-to-face, 50-minute sessions. And suddenly we had Covid and online therapy, before which most therapists would have said, “oh, no, you can’t do that, you’re going to lose everything!”
But the field, and most therapists adapted and realized that yes, you can do good work without being in the same physical space as the client. One thing I hear you saying is the importance of encouraging therapists to be flexible, whether it’s doing art, or standing next to them, or as in the case of “responsive art” where therapists draw along with their clients. However, I can see one challenge in teaching this is encouraging therapists to question their own preconceived ideas of what therapy needs to look like.
JR: I worked in a psychiatric hospital and child guidance center for many, many years, which were part of the University of Pittsburgh psychiatry training program where we trained a lot of social workers, psychologists, and psychiatrists. We discovered that the best way to train people was to get them involved in doing something themselves, even briefly, and then talking to their colleagues about how to use it in their work — just to get a feel for it making something and talking about it. This is the most powerful tool to convince people that it’s useful.
VY: I think of group therapy and how important it is for therapists to have the experience of being part of a group to really understand the power of group therapy.
JR: Same thing with art. I heard this again before the association was founded, from the woman who started art therapy at NIMH, which was one of the earliest places where they were trying it out. She said that whenever you train the staff, to make sure you get them working with materials. That way they will understand what you’re trying to tell them. And I think that’s why I started making films. There’s a limit to what you can tell or say about the arts in therapy with words.
I want to go back to the question you asked earlier about how to help people connect what they’ve done with what’s important to them. You need to be very open and explicit about that. In fact, you can get farther if you work with the symbol, rather than making or asking for any kind of obvious connection, like, “tell me a story about that picture, or what do you think is happening in the picture?”
You can instead ask them questions like, “If you were that person, what would you be thinking? What would happen next? What do you think happened before?” You get them to elaborate on whatever image they’ve created, and then after you’ve explored what they can understand creatively from their own creation, imaginatively, then you say, “gee, so what do you think this has to do with you?” or, “Does this have anything to do with you?
VY: interpreting what their drawing means is an old myth about how art therapists tell the patient what their work means. So, you get them to elaborate on it and tell stories before jumping too quickly to interpret the meaning?
JR: Interpreting what their drawing means is an old myth about how art therapists tell the patient what their work means.
VY: Well, it’s an old myth about therapy in general that the therapist would be the expert and be able to interpret for the client or tell the client what’s happening with them, or worse, tell them what they should do with that.
JR: Exactly! It’s a similar myth. Making the connection themselves is certainly necessary and helpful with older clients and adolescents. I’m not always necessarily explicit with children if you see progress.
VY: Presumably, the clients will often make those connections themselves.
JR: For sure. Once they learn that it’s something connected with them, you don’t need to ask those questions. They just become curious.
VY: I was never trained as an art therapist, but I would keep some drawing materials in my office and occasionally would have the impulse, for whatever reason, to offer that to my clients. And I recall one client drawing with some type of tropical fruit from the country she had come from. She explained that it had this kind of thick, even prickly skin. But inside, there was this sweet, tender, meat of the fruit. And it didn’t it take interpretation on my part to understand that she was talking about herself.
JR: That’s the other thing. The woman who told me to never try to teach psychiatrists without materials, believed, after decades of doing it, that the first drawing is usually a self- representation, even if people don’t realize it. That may never have been tested, and I’m not sure I agree, but it’s often true.
It’s an Artistic Day in the Neighborhood
VY: Changing direction a bit to before you began making videos, you said that you were the Art Lady on Mister Rogers Neighborhood. Can you say a little bit about that, and how that led to you becoming an art therapist?
JR: I was indeed. I was becoming an art therapist while also becoming a child development expert. Fred and I both had the same teacher at the Child Development Center where we worked with the same children. We were colleagues, and students, and workers at the same time. One day he came to me and said, “I’m going to be doing this television program next year and I’d like you to be on it.”I remember saying that I didn’t know anything about being a television performer. He said, “that’s why I want you to be on it, because I don’t want performers — I want real people.” I initially said no because I was going to have another baby and take some time off to nurse. Fred said, “oh, you can nurse before and after the tapings.” He was a little pushy, but I continued to refuse until he said, “don’t you have a grandmother in New Jersey?”
When I told him that I did, he said, “well, the show is going to be shown in New Jersey” — it was only going to be shown on the eastern seaboard in the first couple of years. Then he said, “well, it’s going to be shown twice a day in New Jersey and your grandmother in the nursing home can see you.” I finally and was on about once a month for three years. It was an interesting experience.
VY: What did you learn?
JR: I learned how to adlib (laughs). No, I learned how to figure out what he wanted me to have children do that was related to the theme of his program. But I guess that reminds me that being an art therapist means that you really have to be flexible and creative and figure out ways to work in different environments with whatever sort of person or group you’re confronted with. I ended up liking doing the shows because it was fun and because I was learning a lot.
Around the time I was taping shows with him, I was starting a pilot program at the School for the Blind in Pittsburgh. These were the multiple handicapped blind children, or premature blind babies as they were called at the time. They were being saved in incubators on neonatal units where they had better equipment. They were premature babies who had more than one disability. They were different from “normal” blind children. Sadly, there was a lot of hostility around introducing art with these children — similar to the situation at the Home for Crippled Children, but even more so, because they already had an art program, and said, “oh, you’ll never be able to do anything. These kids won’t be able to do anything.” Of course, it turned out they were. I assessed each child, and of course, they had to be different for blind children. We used a lot of sensory materials.
I said to Fred, “nobody’s ever going to believe how creative these kids are. They are amazing. But there’s such skepticism about them. Even in the school with people who know blind children.”He said, “well, you’ll have to make a movie. I said that I didn’t know anything about making a movie, and he said, “well, you must know somebody with a camera.” That was our conversation. I said that I would ask the people at Children’s Hospital who were already making slides of artwork. They had just gotten a black-and-white 16mm camera and said, “We’d love to go to the school for the blind. We don’t have sound, but we’d love to do it.” It was all very spontaneous, and that was my first film.
Although I hadn’t yet written my first book — I had written articles, one with the director for the Journal of Education for the Blind who said you couldn’t really convey in words how creative these children were. You had to see it. He was right! With seven volunteers, we started a seven-week pilot program, in which we incorporated the artwork with the children. So, we shot on a 16mm and edited on an old Moviola. That was old-fashioned filmmaking, which was fun. That was a new creative process for me, putting the images, sounds, and narration together.
An Art Therapy Film Collection is Born
VY: From there, you went on to create art therapy videos and eventually to curate and build a collection with some of the greatest people in the field, as well as the people who were up and coming.
JR: It was a powerful learning experience, and one that people responded to so emotionally and intellectually, from which they started programs with children like these. It made a difference. I was convinced, and I did get into filmmaking as a way of teaching.
VY: This story certainly resonates with me because it parallels what I did a few decades later. As you may know, I studied with a mentor of mine, James Bugental, who was 80 years old at the time. We kept saying that we needed to capture his work on film, because even though he’d written some brilliant books, it wasn’t the same as seeing someone actually work. He would often demonstrate his therapy through role plays.
I ended up filming him doing a few sessions and released a video, which was the beginning of my journey of creating a vast library of my own. One thing that strikes me about both of our stories is that they start with saying “yes,” and being willing, as you were with Fred Rogers, to then act on the suggestion. That’s the creative process of life — doing something and not knowing how it’s going to work, and seeing what happens. When you’re lucky and it works well enough, you can continue to take another step.
JR: It was for me, as I’m sure it was for you too; it’s another creative process. I found editing films that I created, one of which was about Fred Rogers and his teachings, to be great fun. I would have a hard time separating from it to do my wifely, motherly duties. Putting together image and sound was a way of teaching. Having written a bunch of books, it was a completely different teaching process.
VY: that’s the creative process of life — doing something and not knowing how it’s going to work, and seeing what happensIn addition to creating a number of films yourself, you also put out a call for other art therapists and creative types to send you films that you then curated into the library which you recently handed over to Psychotherapy.net. Hopefully, people reading this interview will be intrigued and want to look. It’s a very impressive and sizeable collection — well over 100 titles. Are there any that stand out or are there even a vignette or scene or two that pop into your mind that you can share with viewers just to entice them? This might give them a sense of some of the riches in the library.
JR: Well, I think for non-art therapists, one of the films that might be most helpful is about children who grieve. I’m trying to remember the title now.
VY: I think that was one that I just watched called “A Child’s Grief.”
JR: It was made in Canada. I got it because I gave a talk at the Toronto Art Therapy Institute where a guy came up to me and said, “I just made a film about people doing art therapy and music therapy; are you interested in seeing it?” He turned out to be a successful documentary filmmaker, but most of the people in that film doing the work were psychologists and social workers. There were also a few art and music therapists who used very clever kinds of instructions to help children deal with the loss of a parent or a sibling. But it was more structured than what I was describing that I would do.
VY: I just watched that and one of the messages I got was how children grieve in different ways. And using art therapy and creative approaches allows them to express that. And obviously, it’s not just children. We all grieve, and live, and emote in different ways.
JR: There’s another film from Canada which I think is inspiring. It’s called “A Brush with Life.” It shows some of the work at a Canadian hospital that had a good art therapy program. It also follows a little bit of a case study of this one woman, who I believe was probably borderline and was having terrible problem. You see her laying down talking to her analyst, but you also see her painting. You also see her in and out of the hospital, and you get a sense of how art played a big role in her recovery. As a case study, it’s inspiring.
I also think that of the two films you decided to distribute, “Art Therapy Has Many Faces,” is a good introduction to the field and is still used a lot. Many people have made subtitles in different languages because it’s an overview and provides a nice history. The other one, “Creative Healing in Mental Health,” shows different art and drama techniques that anybody can use with people of different ages.
Tapping into Creativity in Therapy
VY: Just to be clear, those are two of your films that we had previously incorporated into our collection with your generous cooperation. That was prior to you turning over your entire collection to us, which we’ve published.
So, for folks who are reading this interview and are inspired to learn more about art therapy and bring creativity into their work, are there other general pointers or guidelines or inspiring thoughts you have to encourage them?
JR: To inspire others to explore art therapy, I offer what Fred Rogers said to me about being on television — “Try it, you’ll like it. You’ll be surprised that you’ll find something of value in it.” Maybe start out with mental imagery by saying, “Is there an image that goes with that thought, or that statement, or that idea? After all, mental imagery is something that’s going on all the time and we don’t always paint it, right?!
VY: And that can help unfold inner exploration. Another thing I found is that it can also tell you something about the client that you wouldn’t know through typical verbal conversations. I recall a client of mine who was artistic but worked in commercial art or advertising.
One day, for whatever reason, I asked her, “What goes on in your mind, what do you think about when you’re walking down the street?” It was an unusual question in a sense. What she told me, I’ll always remember. She said, “I’m not really thinking, I’m just observing. I’m seeing patterns of light. I’m seeing colors. I’m seeing shapes.”
It struck me that her inner world was so unique, so different from mine. Most clients, most people for that matter, would never answer that way. Someone else might be thinking or planning about what they were going to do and be excited about it.
Some other clients’ minds might be constantly filled with ruminations or worry about what they had to do or what bad thing could happen. It just always stayed with me to be curious about that, and really drove home the point that every person’s inner world is so unique.
JR: That’s the beautiful thing about art. Whenever I’ve done a workshop with any group, whether it’s teaching or therapy or some combination of the two, the consensus is to use materials in a non-threatening way that are likely to come out looking pretty.
They suggested oil-based clay in different colors — plasticine, which you can get at the drugstore. It’s about fiddling around, warming it up, shaping it without even thinking about what you’re making, or picking three colors, and making something out of it. It’s a kind of doodling it, which reduces anxiety. And when you ask people to place what they’ve made in front of them, it’s as true with clay as it is with doodling, if you haven’t given the topic. The uniqueness of each person is so dramatically illustrated — it’s incredible.
As a side thought, I used to be an art teacher, so for a while I taught some art education classes to people working in elementary and secondary education. I would go to visit them to see how they were doing. For the teachers who were really good at it, their children’s work was engaging and unique. The teachers who were imposing, either consciously or unconsciously, or had their own aesthetic, had children whose work was very similar to each other’s.
VY: In my experiences, many adults don’t think of themselves as being creative, and believe that creativity is about being artistic or being able to do representational drawing. I grew up in an academic family, and was always a little interested in business, but it didn’t seem like a particularly creative field.
But when, kind of by happenstance, I started making videos and then creating Psychotherapy.net, it dawned upon me that the ultimate creativity is about having an idea and creating something out of nothing. There are many types of creativity, but it’s an act of creation, and a conversation like you and I are having.
I may have started with some questions I wrote out just to give me some structure, but as you and I are talking, I don’t know what I’m going to be saying, or certainly how you’re going to respond. I may have some ideas.
It’s going to be entirely unique, but hopefully capture the tension or the distinction we have between wanting to explain and categorize something, versus looking at that same something as a unique or individual expression. Specifically, I’m thinking of the diagnostic process because we are updating our DSM series which contains a variety of clinical diagnostic interviews. It’s been quite an interesting discussion and exploration.
We are exploring the uses, benefits, and the downsides of diagnosis and the diagnostic interviewing process. There’s some benefit to having a common language for communicating with other clinicians. And because there is this common diagnostic language, you can describe someone who is borderline, or depressed, or anxious to someone else, and they will have a clear sense of what you are saying — or at least, that’s the hope. But you also don’t want to get stuck limiting someone by saying something like, “this is your typical depressed patient who has sleep problems with accompanying anxiety. That doesn’t tell the whole picture.
If they do a drawing and you describe the drawing, you’re not going to put it into a category. You’re not going to say, “well, this is a typical, monochromatic scribble with jagged edges.” It doesn’t make sense to think about it that way.
JR: In the early days of art therapy, there was a great hunger for that kind of diagnosis derived from a patient’s artwork. Can you tell this is schizo or manic depressive? And of course, it turned out you couldn’t. Projective drawings were very big in psychology. Maybe you don’t know because maybe it was before you studied.
VY: in the early days of art therapy, there was a great hunger for that kind of diagnosis derived from a patient’s artworkActually, I did my dissertation on the Rorschach.
JR: The Rorschach is different because you’re projecting onto an ambiguous stimulus.
VY: Actually, there is a scoring system which is empirically validated, so I’d say that both are valuable. We need to have some explanations and some common language. But we also don’t want to put our clients’ inner experiences and creativity into a box.
JR: This is my problem with what I call the acronym generation; the art therapists who are now certified in EMDR and CBT. Many of the young art therapists are learning these specific approaches, and they tend to use terms like directive art therapy, which makes me shudder, but that’s a common term. To me, it’s kind of anti-creative, but giving people a theme or a task that’s not bad. Inviting is OK, prompting even, but response art is very tricky. That’s one of the hazards in art therapy, that you have to train the therapists not to project their own ideas onto what they’re seeing, and to know themselves well enough so that they can separate their perception from what is actually being said or created by the client.
VY: And that’s the common issue in all therapies — how to be fully engaged with the client while also being aware of your own feelings and then using awareness of your feelings in a way that’s helpful for the client.
JR: Same idea. Response art has wonderful potential to do good, just like AI, but there are hazards as well.
VY: Just to be clear, can you define what response art is?
JR: I’m not sure who started the term, but Barb Fish recently did her dissertation on it, and it’s become very popular. I’m currently helping my friend, Millie Chapin, a fabulous artist, to sell her artwork online through a mutual friend. A lot of art therapists are actively practicing artists. She worked with Kohut and actually became a self-psychologist who then developed an interesting technique.
She would talk to the patient for a while to find out what was going on, and then she’d say, “Okay, let’s draw about that. I’ll draw and you draw and then we’ll talk.” It was her response to whatever the person told her and then they would talk about both drawings together. When she first had the idea, I remembered commenting that I thought it was dangerous for people who didn’t know themselves as well as she knew herself. But this technique has been embraced by many art therapists because they love using their artist-selves as part of what’s happening. So, it’s not always responding in the sense of actually responding to what somebody’s talked about. That’s Natalie’s technique.
VY: Natalie Rogers, right.
JR: Yes! It’s literally working alongside, which can be quite helpful. I did some of that while I was working with groups of children to inspire a kind of Pied Piper kind of thing. I call that the Pied Piper Effect, because I would start working with the material then they would all start wanting to work with the material. It has an impact when the therapist becomes an important person in the process. And no matter how they try to pretend that they are on equal footing, and that the activity is a collaborative process, clients hope the clinician knows a heck of a lot more than they do.
VY: As we end, Judy, I know we’ve only been able to tap into a small percentage of the stories of your life and your professional development. And as our readers know, or hopefully now understand, you were right there at the beginning of the creation of the entire field of art therapy. You’ve been working since the early 60s, so have had an illustrious career, but clearly, your passion, interest, and curiosity, as far as I can tell, remain as high as ever. And that’s inspiring. I hope that those reading this interview will, by osmosis, feel a little bit of that. And hopefully this will encourage them to learn more about the field, especially by watching the videos you’ve created as they continue their own journeys through life and therapy.
JR: Well, I hope so, too, and that they look at the titles and trailers. It’s much like choosing the art material because there are case studies. There’s work with individuals, groups, families, and couples. So, for me to choose for somebody else what they should watch when you asked earlier, “what stands out,” is hard for me too, because I think it has to appeal to them, and then they’ll get something from us.
VY: Thank you, Judy, for taking the time to share your journey.
JR: Thank you, Victor, for asking.
About Judith Rubin
 Judith Rubin, a pioneer in the field of art therapy, is on the faculty of the Department of Psychiatry, University of Pittsburgh and the Pittsburgh Psychoanalytic Society & Institute. She is a Registered, Board-Certified Art Therapist and a Licensed Psychologist. Dr. Rubin is the author of five books, including: Child Art Therapy, The Art of Art Therapy, and Art Therapy: An Introduction. She was the “Art Lady” on Mister Rogers’ Neighborhood in the 1960s
Judith Rubin, a pioneer in the field of art therapy, is on the faculty of the Department of Psychiatry, University of Pittsburgh and the Pittsburgh Psychoanalytic Society & Institute. She is a Registered, Board-Certified Art Therapist and a Licensed Psychologist. Dr. Rubin is the author of five books, including: Child Art Therapy, The Art of Art Therapy, and Art Therapy: An Introduction. She was the “Art Lady” on Mister Rogers’ Neighborhood in the 1960s