Compassion is the basis of morality.
—Arthur Schopenhauer, The Basis of Morality
Should you have to treat people who have assaulted or murdered others? What about working with clients who hold hateful beliefs or taboo fantasies or act in ways that directly contradict your moral standards? What if they’re blatantly sexist, racist, homophobic, or transphobic? How do you know what your role is when you feel disgusted or angry or upset by how a client lives their life?
All humans are unquestionably shaped by their values. No matter how much you try to embrace your open mind, some implicit biases are inescapable. Everyone has preconceived criteria for which behaviors feel acceptable or unacceptable.
Therapists often work with people the rest of society often belittles, misunderstands, and ostracizes. When a client sees only the bad in themselves, you reach in and find all the good. You hold a light in a place that can feel so dark.
But what if you don’t like the client? What if you not only disagree with their values but find their personality annoying or obnoxious? What if some or all of their mannerisms irritate or upset you? What if you find yourself feeling agitated during your work together?
Let’s slow down here. We invite you to spend a moment thinking about a value you hate. Hate is a heavy word; we chose it because it triggers strong emotions. For example, maybe you hate self-centeredness or people acting like they know everything. Now imagine you have been assigned to work with a client who holds or embodies these specific traits. They show no interest in changing, but they’re in a state of distress, they need help, and you have the expertise to help them.
Could you do the work? Could you genuinely support this client, find their goodness, and be on their team? In everything you do with them, could you commit to caring about their well-being?
Feelings of dislike exist on a large spectrum. Unfortunately, you may not be prepared to manage it when it happens. Negative countertransference arises when we experience conscious or unconscious negative reactions toward a client. Despite the word negative, these feelings are not good, bad, right, or wrong. But we must be mindful of how they can affect treatment. Acting out as a result of negative countertransference can include:
- Rejecting your client
- Offering unsolicited advice
- Avoiding certain topics because they make you feel uncomfortable or unsafe
- Openly disapproving of your client’s choices
- Withdrawing from emotional connection
- Being defensive or dismissive of your client’s feedback
- Demonstrating inconsistent boundaries throughout treatment
- Trying to overcompensate for your dislike by being overly agreeable or passive
- Prematurely abandoning a client due to your own frustration or hostility
Negative countertransference sometimes happens when a client inadvertently knocks at unresolved parts of your own life. Maybe their anger reminds you of your father’s anger, and you have a contentious relationship with him. Maybe their passivity speaks to your own difficulty asserting yourself, and you resent having to be the strong communicator in the relationship. Perhaps you’re an unpaid intern and aren’t sure if you can make rent this month and your wealthy client is lamenting about their next real estate venture. Because you are a human and not a robot, it would make sense if you felt agitated by these circumstances.
There are no bad clients. But some clients may feel bad for you. In addition to unpacking personal reactions in therapy and supervision, here are some guidelines for managing your emotions and offering helpful and ethical care to your clients. We explore them in more depth in the subsequent sections.
Managing Your Emotions in Therapy
Leaning deeply into unconditional respect: Deliberately choosing to respect your clients for who they are, where they are, and what they bring to you
Deliberately searching for the good: Intentionally finding and holding on to your clients’ strengths and virtues
Embracing empathy as a nonnegotiable: Prioritizing a warm, empathic approach with your clients regardless of your similarities or differences
People are just as wonderful as sunsets if you let them be. When I look at a sunset, I don’t find myself saying, “Soften the orange a bit on the right-hand corner.” I don’t try to control a sunset. I watch with awe as it unfolds. —Carl Rogers, A Way of Being
Respecting clients means fully accepting them for who they are and where they came from. It entails honoring where they stand in their current journeys.
Respect moves into valuing autonomy. Clients have the right to live their own lives and make their own choices. You can have your opinion, but you do not live in your client’s body, reside in their home or community, or manage their relationships. Respect is the prerequisite for unconditional love. And love can be such a rich part of therapy, even if you don’t identify with loving your clients in the specific sense of that word. Respect is also a catalyst for helping you release rigid expectations about how a client should think or behave. This opens deep space for curiosity and connection.
Respecting clients does not mean condoning problematic behavior. We’re not advocating clients harming others or themselves. We absolutely want to see people make optimal choices in their lives.
However, respect means seeking to connect with the context and motive driving someone’s behavior. As a species, each person’s way of being is influenced by so many factors, including their culture, geography, upbringing, family influence, neurobiology, trauma, and genetics. It is especially important to remember this when working with clients you find challenging.
Respect can get muddled if you struggle with believing your clients owe you something. For example, therapists sometimes believe that clients owe them:
- Complete honesty
- A desire to do deep work
- The belief that therapy is a worthwhile investment
- Motivation for growth
- Insight into their current needs or problems
- A full understanding of therapeutic boundaries
- A willingness to integrate feedback
- Socially acceptable behavior
- Measurable progress
Having some parameters for treatment is reasonable. You are hired to support your clients to achieve specific mental health treatment goals. This work should adhere to certain protocols; deviating too far from the basic structure of therapy can create problems. However, treatment in the real world does not exist in a predictable cut-and-paste formula. Clients come to therapy with unique personalities, unmet needs, and distinct behavioral patterns. Many arrive in a state of crisis when other resources have proven to be unreliable or unavailable. If they are mandated to therapy, they might resent having to meet with you altogether. In almost all cases, clients are juggling numerous stressors, and they want relief from their distress.
Respect helps therapists mitigate the risk of inappropriately generalizing or stereotyping clients. For example, let’s say you conduct an intake with someone who discloses a horrible experience they had with another therapist in the past. They express their anger toward the healthcare system and tell you they have doubts that you can help them. Some therapists would flag this client for being “too difficult,” or even, “treatment resistant.”
Respect means you give the client the benefit of the doubt. You listen to what they have to say about those past experiences. You care about their pain, and you emphasize that you care about that pain because you value their wellness.
As a therapist, respect means you hold the CHAIR (consistency, hope, attunement, impact, and repair) model as much as possible. You strive to convey a positively consistent presence for your clients. You find and hold on to hope for change in every way you can. You seek to attune to their emotions and needs. You look for opportunities to impact them and help them experience their world differently. And if and when conflict occurs, you take the lead in repairing that discourse.
Respect also means truly owning what lies in your locus of control. This, too, is covered by CHAIR. Ultimately, you can control the knowledge you obtain, the therapeutic actions you take, and the presence you exude. You control the boundaries you set, how you advocate on behalf of your clients, the referrals you provide, and the way you acknowledge making a mistake. Depending on your specific workplace setting, you may also control many logistics, including your fees, documentation protocol, after-hours contact, intake paperwork, and the arrangement of furniture in your office.
In reality, however, you can do everything you’re clinically supposed to do, and you still can’t control your client’s reactions. You aren’t in charge of deciding whether you have rapport. You can’t fix whether a client’s partner loves them or whether their boss perceives them to be incompetent. You can never control what a client does or does not do within the context of therapy itself.
The good news is that the more you can respect your clients, the more meaningful this work feels. This is because when you have a foundation of respect, you can lean more deeply into the caring part of this work.
We believe it’s impossible to care too much about a client. To care is to be invested in someone’s well-being. When you care, your heart and soul come into this work. It is one of the most beautiful traits you can bring to clients. As for us, we care about our clients immensely and wholeheartedly. We also have no qualms about telling them we care. We want them to know they are worthy of being cherished because they are. Holding this privilege gives our work such vitality.
Caring is not the same as enabling, overextending, or breaking therapeutic boundaries, however. Those specific actions often come from a place of caring, but they might speak more to unchecked countertransference when therapists lose professional objectivity and presence.
Caring lends a hand to respect, allowing you to detach your compassion and tenderness from expectations. Within this state of respect, you genuinely want what feels best to your clients without defaulting to an assumption that you know what’s best for them. You can value rapport and connection without ever demanding it. Most of all, you can and should care without conditions.
From this lens of respect, therapists can trust how the process of therapy organically unfolds. The freedom lies in the flexibility. It is the balance of accepting clients for exactly who they are while holding on to the hope that change can always happen.
Therapy, from this framework, bursts with possibilities. Embracing radical curiosity sets the stage for holding unconditional positive regard for your clients.
You won’t agree with or like every client you work with, but respect means trying to understand that most everyone is doing the best they can in a given situation. People want to secure their survival. Clients seek to avoid pain, even when that means hurting themselves or others.
How You Cultivate Deep Respect for Clients
Prioritize curiosity at its utmost capacity: What past circumstances led this client to make the choices they made? How, in every moment, are they seeking to minimize pain? Which behaviors have become solutions to temporarily cope with distress? Who hurt them and created those unhealed wounds in the first place? How are they trying to do the best they can with what they have?
Check in with yourself when you think a client owes you something: Be mindful of the tendency to assume your client inherently owes you something. If you find yourself struggling with this, ask yourself, Why do I find this so important? If you’re struggling to let go of this expectation, practice saying to yourself, How can I meet this client exactly where they are?
Focus more on what you owe your clients: You owe consistency, hope, attunement, impact, and repair. You can’t control how your clients respond to what you offer. Leaning into your locus of control may help release the demands you feel toward clients or the treatment itself.
Pay attention to your countertransference: Countertransference is not good, bad, right, or wrong. It exists and can’t be avoided. But you can be mindful of how you orient treatment when it arises. Remember that your client, even if they remind you of someone or something you dislike, is a whole person with a distinct personality. Remind yourself often of this aspect of therapy.
Commit to neutralizing your values within therapy: In your personal life, you are entitled to orient yourself in ways that honor your values. But your job as a therapist is to show up and support your clients with respect, compassion, and professionalism.
Allow yourself to care tremendously: You are allowed to care about your clients. You are allowed to have feelings of protectiveness, adoration, warmth, delight, and closeness with the people you work with. Deep care, of course, should not justify consistently breaking therapeutic boundaries.
Have a plan if you simply cannot set your negative reactions aside: Sometimes this happens. You may not be able to work with certain clients because their content is too triggering to you. This does not make you a bad therapist. However, it’s in your client’s best ethical interests to refer them to a provider who can competently treat them. If this isn’t possible, focus on getting quality supervision, consultation, and/or personal therapy to address your issues.
Deliberately Searching for the Good in Clients
As therapists, we are called to search for the good, even when the good feels buried or insignificant compared with other traits we see in our clients.
It is also imperative to remember that no value is unanimous. As the philosopher Friedrich Nietzsche said in his book Beyond Good and Evil, “There is no such thing as moral phenomena, but only a moral interpretation of phenomena.” Humans have decided on some parameters of good and evil, but a choice that feels boundlessly immoral to one person may be entirely warranted to someone else.
If you assume a stance of moral superiority, you risk operating from a “me-versus-you” mindset. This mindset can create competition, and competition erodes the fabric of the relationship you’re trying to build. If you aren’t on the same team, you unknowingly risk becoming opponents. You may feel irritated, offended, and riled by your client. Your client may feel judged, condescended to, or unsupported. You both are apt to move into defense stances—and this defensiveness may prevent the crucial scaffolding of emotional intimacy from developing.
Your work as a therapist means signing up to care about people who think and act differently than you do. Biases are inevitable, but you must be able to examine inward and dismantle feelings of superiority. You are not a savior. You are not the all-knowing expert. You have simply been invited into a sliver of your client’s life. You owe it to them to witness their pain and understand the gravity of their life story.
Searching for the good means assuming a stance of giving clients the benefit of the doubt. This becomes especially important when working with clients who feel challenging. When you can pause and drop into a client’s pain, when you can land into the rawest feelings and deepest wounds, you soften. There are many ways for therapists to soften, but it happens when the therapist can truly land and sit with someone else’s emotions, no matter how big, heavy, or confusing they are.
Softening is the catalyst for opening. Opening emotion, opening trust, and opening connection. Everyone needs a soft place to land, and you have the opportunity to create this place for your clients. Not all will take you up on it. But many will.
Your expertise isn’t what makes therapy meaningful. Your courage to move beyond societal constraints and listen to another person is part of your impact. It’s a deliberate choice. But in our judgmental world, you are privileged to make this choice every session.
It is tempting to find out what is wrong with your clients. The reward of this work comes from uncovering what is wholly good.
Embracing Empathy as a Nonnegotiable
Empathy refers to the capacity for relating and sharing feelings with another person. It means being able to sense what someone might be experiencing and hold space for that experience. When someone feels empathic, they feel warm, and people tend to be drawn to the energy of warm people.
What person comes to mind when you think of the word warmth? It may or may not be a therapist, but it’s certainly someone who feels highly approachable and friendly.
Those who exude warmth demonstrate how much they care about people, and this care is felt through their words and actions. They tend to be optimistic without being overly positive. They remember details and they understand pain. They know how to hold emotions without overreacting or underreacting. You want to be around them because they feel safe, and that safety feels good.
Some people mistake empathic therapists for naive therapists. This, however, is rarely the case. Truly holding empathy without constraints means understanding and making space for all the mistrust, skepticism, and shame that people who walk into therapy carry.
Instead of condemning or withdrawing from those barriers, empathic therapists simply make space without any pressure or judgment. They respect the client’s defenses for their necessary function. Empathy is patient, and empathy doesn’t have an agenda.
We encourage therapists to self-assess their empathy by ranking themselves on a scale from 1 to 5 for each of the statements listed below:
1 = almost never
2 = rarely
3 = sometimes
4 = often
5 = almost always
1. I seek to understand a client’s pain deeply.
2. I consider the context of why someone might think or act in a certain way.
3. I can imagine what life feels like in my client’s shoes.
4. I am told I am a great listener.
5. I am told I am warm or kind.
6. I consider myself to be exceptionally compassionate.
7.When I think about my most difficult clients, I would rank myself as having an extraordinary amount of empathy for them.
8. I do not expect people to change on my behalf.
9. I am patient with relapses, regressions, and setbacks.
10. I believe I can genuinely sit with another person’s emotions well.
You want to strive for a score of 40 or more. If it’s lower than that, consider deliberately practicing more empathy in your work or asking for help if you are struggling with a particularly challenging client. Like any muscle, our capacity for empathy needs to be worked out regularly to build strength. But the stronger it is, the more you will connect with your clients and respect them for exactly who they are.
Guidelines for Softening and Finding the Good
Imagine your client’s younger self: Your client’s present self is a product of millions of interactions and experiences. The “challenging” clients are often the ones who have experienced extreme hardship earlier in their lives. When you can drop into noticing their younger state, you will likely find it easier to hold empathy. For instance, instead of solely seeing a client as an angry, self-righteous man, you can also see the part of him who is a fearful and helpless little boy.
Look past diagnoses and symptoms: Diagnoses are theories that summarize a given set of presenting behaviors. Even if you accept a diagnosis, everything is subject to scrutiny and change as humanity evolves. It is imperative to push past limiting thoughts such as believing that someone with panic disorder or someone with schizophrenia automatically behaves a certain way. Diagnosing can be a helpful starting point, a tool, but it is never an end point. It does not paint the full picture of who someone is, what they struggle with, and what they need to move forward.
Practice more mindfulness: Slow down in session. Be more deliberate with how you listen and understand your client. If it’s helpful, consider entering a potentially challenging session with the intention, I will look for what’s wonderful in this person. When this notion is your compass, you seek to find strength and goodness.
Remember, everyone is trying to survive: This stance can’t be emphasized enough. Recognizing this truth is not the same as condoning any specific behavior. Rather, it offers an understanding of why people develop certain patterns, no matter how destructive.
Prioritize empathy: Although empathy is often taught as a preliminary skill in graduate school, it’s not a pervasive trait among all therapists. If you struggle with experiencing or manifesting empathy, focus on what might be in the way and, over time, prioritize implementing more empathy in your work.

.jpg)
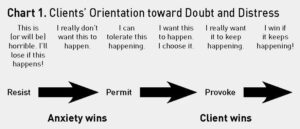
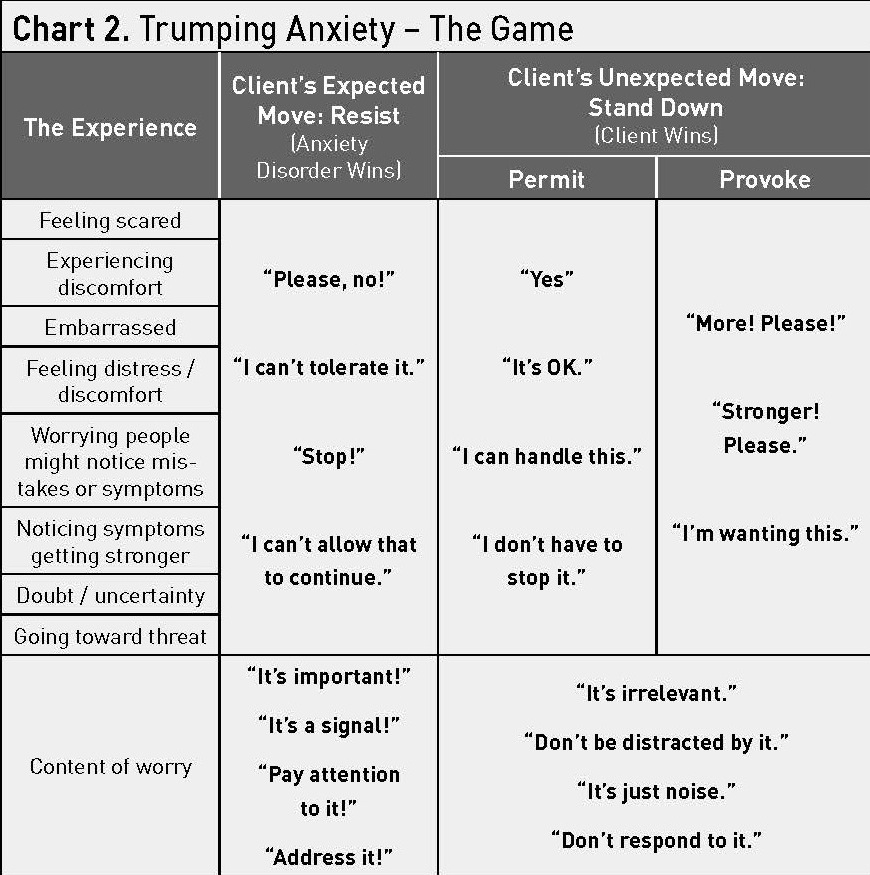
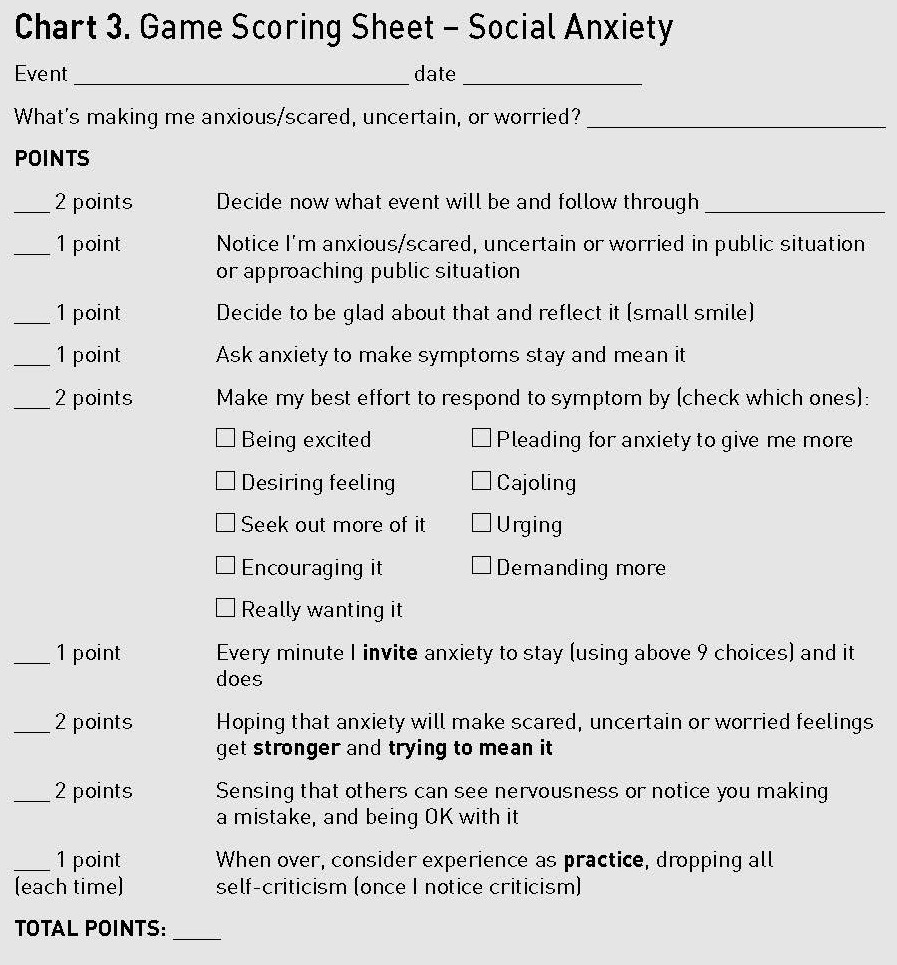 As you review Chart 3, you can see the essence of the provocative game and the weight of each type of activity. These illustrate the goals I want them to set during practice. They reflect the essence of paradoxical action in fearful situations:
As you review Chart 3, you can see the essence of the provocative game and the weight of each type of activity. These illustrate the goals I want them to set during practice. They reflect the essence of paradoxical action in fearful situations: