Learn how to see. Realize that everything connects to everything else
— Leonardo Da Vinci
The internet in the late 1990s was exciting because you could research topics including sports, education, and entertainment and stay in contact with old friends. In retrospect, however, when working with adolescents at a local PHP and IOP, I/we ignored the impact of Myspace and other social media websites that encouraged cutting and suicide. We attributed the increase in behavior to peer influence and the impact of dysfunctional family relationships.
Today, social media’s algorithms and influencers have more of an impact on the family than we are willing to acknowledge. It has been argued that social media’s algorithms entice family members who use social media to spend more time on the app than with their own family or friends. As a clinician who works with families in private practice and schools, it has become increasingly clear to me that social media’s algorithms and influencers often occupy the “empty chair” in the family sessions.
The “Therapeutic” Power of Influencers on Family Systems of Care
It was evident to me while watching the hearings in Washington, DC a year ago that social media companies will not change their algorithms and will not share them for everyone to understand. The Netflix documentary The Social Dilemma had many former social media employees expressing eye-opening concerns. The film revealed how tech companies hire psychologists to make a persuasive algorithm to increase the appeal and use of their apps.
Unfortunately, Congress appears powerless, unwilling, or both, to make changes due to the powerful lobbying groups. Some have said that Congress is waiting for the UK’s Parliament to take the lead in regulating this industry.
Social media makes money by showing images or comments that their algorithms “say” are interesting and encourage consumers to “like,” “comment,” or “share.” Social media companies have also learned the more divisive and inflammatory the post, the more views and money there is to be made.
Well-designed apps continually boost the user’s connection by showing information, comments, or images that they have discovered are of interest. Showing an opposing view or people from a different “virtual tribe” will decrease the views/time spent on the platform and decrease money for the makers of the app. The app creates a virtually closed system that does not allow any “disliked” information or contradictory views.
If different members of a family “like” different apps, or different posts on the same app, each member of the family may conceivably align with a virtual presence against their actual brick-and-mortar kin or friend. As a result, algorithms have the power and potential to intensify the already-present pattern of conflicts within a family system or relational circle. Disconnection, chaos, conflict, and exacerbation of individual and/or family pathology may follow.
Influencers have always been present in our society. For many years, our influencers were teachers, family members, neighbors, friends, supervisors, actors, news anchors, and other people in our community. We would ask our immediate community personal and embarrassing questions. Many times, adolescents and young adults would get personal and difficult questions answered by building up the courage to approach someone face-to-face in their community.
Building up the courage to ask questions taught us how to manage our fear and anxiety. Navigating face-to-face relationships also teaches us how to manage embarrassment, frustration, anger, resentment, and rejection which is an important step in our development. Non-virtual relationships also allow us to feel emotional and physical closeness that is missing in social media/virtual relationships.
Today, our society is teaching the belief that anxiety is a bad thing that needs to be kept at bay. We in the field know that anxiety is not the problem. Arguably, anxiety is a result of the person’s core belief and/or what is going on in a relationship that will not change for the better. Because of this, adolescents and young adults are narrowing their non-virtual relationships because it is the path with the least amount of risk.
When asking intimate or difficult questions face to face, we learn how to manage proximity and closeness in our family and friend groups. We learn who in our family and friend groups has earned the privilege to be asked these intimate questions. We learn who can keep our personal life private and who may have the better answer, which builds friendships and family relationships.
Social media triangulates family and friends to find the immediate answer and connects people to a tribe that challenges them the least. Many believe decreasing their non-virtual relationship decreases their anxiety, but it actually increases their isolation from their community and increases their anxiety when meeting someone face-to-face. Also, virtual relationships give the illusion that all of these important ingredients are present on social media.
Family members are turning to influencers as if they are therapists/experts with answers (good therapy doesn’t give answers.) Or they are turning to politicians that they must blindly follow (good politicians allow debate.) We know the politicians who are at the extreme right or left posting inflammatory statements get the most views.
These influencers are making statements encouraging family members or friends to pick sides, skipping the process of face-to-face discussion with follow-up questions or reflection that occurs in non-virtual relationships. When a person stops exchanging ideas with their family members or friends, it creates a dangerous virtual closed system.
During my training at the Minuchin Center for the Family, I was always asked, “Whose shoulders is the adolescent standing on?” One year, a family I was working with agreed to meet with Dr. Minuchin for a consultation. Dr. Minuchin said to me after the consultation, “You will fail because the system of care erodes the boundaries of the family.” It became evident that each of the six members of the family relied on their own individual therapists to reinforce their view of how everyone else in the family was toxic.
This taught me the importance of understanding the family map in addition to evaluating if different family members were in coalitions with other therapists, social workers, and/or even agencies. It was an important step to understanding the map and identifying where the coalition(s) across generational boundaries occurred with the family and larger system.
In many of the sessions, other families were able to overcome their symptoms once they began to work on their relationships and change their relationships with the systems of care. It was exciting to see when the system of care noticed their triangulation with the family. Other times it was sad to see how systems of care did not see how they were triangulated against family members.
Today, influencers are present in the family session as seen by the virtual coalitions that the member(s) must maintain as if they were their closest friends in order to be a part of their tribe/team.
The Impact of Social Media on Family Relationships
Families are always ahead of the researchers and therapists, but do we listen to the pieces together as therapists? The following are the themes/symptoms families have discussed in my own family therapy sessions as well as those of colleagues in the wider clinical world. Each of these impacts adolescents, and, in turn, how they impact the adults in their home. On both sides of the relational equation, social media has a powerful impact, and not always for the good of individual and shared relationships.
When one or more family members are engaging in excess screen time from two to sometimes more than six hours a day on social media, the research shows there is an increase in symptoms of depression and/or anxiety. If someone has this much daily screentime, they are displacing healthier activities or hobbies such as walking, sleeping, drawing, painting, mindfulness, and gardening, to name but a few. And this displacement impacts the interactions in the family and community by isolating them.
Algorithms encourage constant social competition and comparison, and as such function as social currency between peers and family members. Adolescents typically feel that they are on stage competing to increase their position in the “hierarchy” with peers and/or parents. They continually compare themselves to peers at school and other families.
The algorithms that draw them in make it difficult for them to turn off the social app and get away from the stresses of adolescence. Jockeying for competition and comparing their lives to others may at times backfire, leaving them feeling poignantly and painfully alone. Again, this constant competition and comparison mirrors similar interactions in the family that can contribute to increased anxiety and depression.
The adolescents I’ve worked with discussed how they feel lonely and alone. They feel lonely when they are not supported or perceive they are not supported by family or friends, and feel alone when they have little face-to-face contact with peers like we all experienced during COVID.
The two-dimensional views people experience when using Zoom as the primary source of connection do not “feed the soul.” There is no substitute for good eye contact and close physical proximity. The irony is social media was created to decrease feeling lonely and alone but actually amplifies it. In family sessions, many, if not all, talk about how they feel lonely and hoped that social media would fill this void but were unsuccessful.
Adolescents typically think they are invisible or always on stage. These polar positions can occur on the same day for any adolescent. They think they are invisible when they are spending more time on their phones not getting enough likes and/or views, whatever that means to them.
This causes them to work harder on their online stories and identities, decreasing the proximity with their non-virtual friends. Many adolescents begin to look for the “genuine” or “real” friends, determining they are only present in social media and not in their own hometown or within the family walls. In the family, these themes are very common when there is already a pattern of disengagement (invisible) or enmeshment (always on stage).
The adolescent also thinks their peers are waiting for them to make a mistake so it can be posted online. This position makes them feel as though they are always walking into the cafeteria for the first time as a freshman in high school. Adolescents are supposed to make mistakes, struggle, learn about relationships with typical external distractions (friends, family, media, work, and politics). But does social media fill the lonely times when the adolescent and young adult are reflective and recoup?
Being invisible or always on stage prevents the adolescent from developing close connections with peers, teachers, coaches, or other family members. This results in adolescents seeking temporary relief from asking a “person” and instead getting information from social media.
Information on the app is monitored by the algorithm and is not as embarrassing or stressful as asking a family member, friend, or teacher. This is where social media begins to enter the family, impacting the adolescent development and challenging their family’s belief system.
The algorithm also motivates the adolescent to seek select information that aligns with their narrow/closed view about politics, friendship, religion, sexual identity, sexuality, gun laws, suicide, mental health, or any other hot topic.
The Atlantic, 60 Minutes, Pew Research, the New York Times, and the Wall Street Journal have done a great job discussing all the different ways social media has triangulated members of our families. The New York Times article on suicide, “Where the Despairing Log On and Learn Ways to Die,” by Megan Twohey, or The Wall Street Journal essay, “TikTok Diagnosis Videos Leave Some Teens Thinking They Have Rare Mental Disorders,” by July Jargon are exemplars.
Social media focuses on the “person” and navigating them to topics they are interested in and picking what tribe to belong to. The information is flowing into one part of the family system and not to the whole family which triangulates family members against virtual friends or influencers. This occurs if the family is already in a state of constant conflict or conflict avoidance. A recent 60 Minute piece discussed how China does not allow TikTok to bring up divisive topics to their children or adolescents.
For the adolescent to decrease feelings of anxiety and depression, they must work for the “likes” and “views.” They will be trying to affirm their sense of self, but many times they will be accused of bragging and will feel they are not good enough when comparing or competing with others.
Body image and feeling unattractive are especially amplified by social media’s filtering app. Many plastic surgeons are reporting an increase in adolescents wanting to get surgery to look like their filtered self. Current data shows that 55% of surgeons report seeing patients who request surgery to improve their appearances in selfies, up from 42% in 2015. They want fuller lips, bigger eyes, and smaller noses. “This is an alarming trend because those filtered selfies often present an unattainable look and are blurring the lines of reality and fantasy.” (1)
When I’ve met with families and these themes come up, I have encouraged them to discuss these themes which have allowed me to see the systematic position of each family member, system of care and the influencer/algorithm.
Every family has its struggles and at times feels out of control when it goes through a stage of what Monica McGoldrick calls its family life cycle. I have seen this especially when a family enters my office as it is attempting to (re)adjust to the needs of their childhood, adolescent, or young adult. Now add the influence of social media to one or all members of the family, the spiraling becomes more intense.
Crisis of Voluntary Play for Children
The importance of free and voluntary play with children to teach them how to give and take has been well documented. There is no substitute for non-virtual relationships in the early stages of childhood. Antithetical to this, algorithms require constant attention, taking the time away from connecting with others face-to-face.
Whether it is the child who requests to go on the smartphone or the parent who gives the child a cell phone in social situations (i.e., play dates, restaurants, long car rides, it decreases the opportunity to negotiate, argue, entertain themselves, compromise, and resolve conflict. This “tech choice” leads to delaying the development of the family and prevents them from moving to the next stage of a family with an adolescent.
Children Entering Adolescence Have Not Learned to Play
There comes a point in families when adolescents are told they are no longer a child, yet neither are adults. For some adolescents, not knowing the initial stages of voluntary and free play puts them into limbo looking for answers. The adolescent and family know on some level they are missing the tools for non-virtual relationships.
First, this is where the social media’s algorithm and influencers potentially intensify the family’s struggle. When the adolescent looks to social media for the answers, this intensifies conflict. Naturally, the adolescent wants to grow away from the family. They want to connect more with peers.
The adolescent in families with intense enmeshment/disengagement and different forms of coalitions struggle the most. This is where social media’s algorithms direct the adolescent to find a group. The algorithm pulls the adolescent in to spend more time on their app, resulting in the app making money and the adolescent searching for connections separate from the family.
However, virtual connections encourage the same patterns of enmeshment/disengagement and the different forms of virtual coalitions. These intense virtual connections are sometimes in opposition to the non-virtual relationships of the family and/or community.
Secondly, this social media generation has grown up learning to communicate more virtually and less in person, especially during COVID. Many adolescents have decided that they would rather communicate virtually. It is hard for some adolescents to look into someone’s eyes, read body language, and feel the energy of being in proximity because it makes them anxious. Look at any lunchroom at any local high school. If the school allows students to be on their phones during lunch, adolescents prefer to spend time on their phones working to maintain a social virtual hierarchy.
Social media offers a prime context for navigating these tasks in new, increasingly complex ways: peers are constantly available, personal information is displayed publicly and permanently, and quantifiable peers’ feedback is instantaneously provided in forms of ”likes” and ”views.” (2). Many of us who grew up before social media can only imagine if our mistakes were on a permanent record and followed us around for the rest of our lives, never allowing us to move forward.
Thirdly, the family does not have a chance to limit the adolescent’s time on the apps because the social media’s algorithm encourages constant attention, reinforces isolation from family and non-virtual friends.
Many parents have approached me saying, “The phone is their lifeline to manage their anxiety,” or, “The phone is the only way they connect with their friends.” During these moments, I have found it useful to explore how the whole family has come to the belief that the social app has become a way to maintain the homeostasis of the family.
A Non-Virtual Family Map
I often ask families about their virtual and nonvirtual family maps. I think it is important that we ask the family about their social media involvement to understand the virtual map of the family. Do families understand the impact of the social media algorithm? Do families know how to get out of the social media web? Do we ask each member of the family who they talk to virtually or non-virtually when they are struggling?
In initial evaluations, I often explore if the family is aware of how many hours they are spending on the social media apps. It is important to assess if the family is aware of how much social media raising/influencing is involved in the marriage, parenting, and sibling subsystem. Some providers want to focus on social media addiction, but the algorithm is not like any other “addiction.”
The algorithm allows many of the family members to covertly — and sometimes overtly — bring influencers into conflict with different members in the family. These virtual relationships amplify the family’s symptoms, and unfortunately today’s therapists use the medical model to diagnose the adolescent symptoms, further pathologizing and pushing the relationships in the wrong direction. This narrow view further sets the enactments, reinforcing the enmeshment, disengagement, and coalition patterns.
Non-Virtual Family Map
It is hard to shift our medical model training from a focus on the individual’s (child, parents, siblings) deficits to one that acknowledges strengths and competencies within individuals and the family system. When individual therapy does not make significant change, families often turn to family therapy as a last resort.
After experiencing this different approach, they often express frustration that they were never given the opportunity to move forward together, instead deferring to the experts for the correct intervention and diagnosis.
Structural Family Therapy was so different in the 1970s and 1980s; it was transcendent. While many new theories of family intervention have reached the mainstream, so too have many reverted to focusing on the individual. When starting individual therapy with the adolescent, I have found it important to ask the adolescent to overcome the algorithm on their own without their parents’ involvement. As family practitioners, we need systemic thinking more now than ever to approach the intense cultural impact of algorithms and influencers.
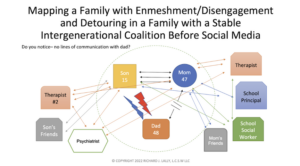
Below is a “traditional” family map that does not consider social media. It represents a compilation of families I’ve seen in therapy, rather than any one family. The symptoms include those typically seen in family practice — poor school performance, school avoidance, vaping, drinking, and using drugs.
From a system’s orientation, the symptoms are a result of the functional and dysfunctional interactions within the family system.
.png)
It’s hard for me to understand how therapists begin assessment and treatment without considering or involving the whole family. Some clinicians might say the conflict is too high, and it would only impact the adolescent negatively. Others might assume from the start that one or both parents are not willing to work or are too busy. Some might even be unaware of the importance of beginning from the position that families do not have the strength to make change.
Sometimes therapists and school staff buy into and reinforce the belief that the child or teen is the problem. In the case of this particular map, Mom “reportedly” goes to her private therapist while the son sees his own therapist. Mom and son separately complain about dad to their respective therapists and to the school staff. When mom and son voice frustration about dad and each other in the individual therapy session, disengagement with dad is reinforced. Mom and son are trying to get the type of connections from the system of care that they cannot get with Dad.
While this disengagement takes place, the son turns to his peers, attempting to pull away from mom’s enmeshment, activating her to pursue more. At home, Dad complains that his wife and son always bring up their therapist who agrees that he is unavailable and/or flawed. When this occurs, Dad becomes more distant and angrier, feeling like he is the odd person out.
When Mom gets angry at dad, she turns to her son and vents to him which activates him to challenge his father about money, drinking, and the way he treats her. At other times, the son may jump into the conversation when the parents interact about money, drinking, or the way he treats Mom.
When I attended graduate school, the common exercise was to map the triangles in the family system. Based on the above map, there are at least 24 triangles that are activated in the family-school-mental health system. The 24 triangles are:
- The mom, son, and dad
- The mom, son, and school social worker
- The mom, son, and principal
- The mom, dad, and school social worker
- The mom, dad, and principal
- The mom, dad, and school social worker
- The mom, dad, and school principal
- The mom, son, and mom’s friends
- The mom, dad, and mom’s friends
- The mother, dad, and dad’s friends
- The mom, son, and son’s friends
- The mom, son, and son’s therapist
- The mom, son, and son’s psychiatrist
- The mom, dad, and son’s psychiatrist
- The mom, son’s therapist, and psychiatrist
- The mom, dad, and son’s therapist
- The mom, school social worker, and mom’s therapist
- The dad, son, and son’s therapist
- The dad, son, and son’s friends
- The mom, son, and mom’s therapist
- The mom, dad, and mom’s therapist
- The son, son’s therapist, and school social worker
- The son, son’s therapist, and psychiatrist
- The son, school social worker, and principal
These 24 triangles are at the same time difficult for adults in the family to appreciate, even harder for an adolescent, and deeply challenging for the clinician to manage. In those triangles within the family where cross generational coalitions are activated, the symptoms in the family increase. I have often been challenged whether to discuss the impact of all these cross generational interactions with the family and whether it is important to differentiate the healthy, less healthy, and unhealthy ones from each other
On top of the above complexity, other questions arise like “where did the boundaries go?” The therapist must keep in mind how the boundary between the family and the outside world becomes invisible and the symptoms become more intense, to the point more professionals are recruited to “fix the dysfunction.”
I have also had to maintain awareness of how managed care’s enforcement and reinforcement of the medical model has influenced me and other members of the community of care, including other therapists, psychiatrists, physicians, and schools. This reinforcement has an impact on the family’s interaction with the son focusing only on his diagnosis and the correct medication, while failing to address the family relationships.
As mom turns to the school and the system of care for answers, things are not changing. She reports that her son is getting worse. Mom blames dad’s aloofness and dad blames mom’s overindulgence. Mom increases calls to the psychiatrist. The psychiatrist adjusts the medications frequently. The frequency of crises increases and the boundaries between the family and the outside world are dissolving due to the interaction between the family and the system of care.
The number of alliances increases between different family members and different professionals as more professionals/agencies are pulled into the drama. Professionals unintentionally begin to write/rewrite the individual’s and/or family’s stories, especially when utilizing the medical model.
With more stories, there are more opposing interests for each family member. This phenomenon between families and agencies is a result of a collision when both parties collaborate to uphold sociocultural trends. The goal is not only to interrupt multiple unhealthy alliances with existing professionals/agencies, but to also prevent new transactions from developing. (3)
This phenomenon was usually seen when the system of care worked with economically challenged families. We now see this also occurring with families of significant means because they can afford an individual therapist for each family member and psychiatrist(s) if needed.
As we look back at the map, it is now easier to understand that because the family has already identified what they think is the problem, it really needs to address the triangle between mom, dad, and son. It doesn’t really matter where to begin. A clinician can enter through mother-son enmeshment and coalition, father-son disengagement, or parental/marital disengagement.
It might also be useful to address the system of care coalitions between the therapist and school with the mom and son. Having the family identify how to change the interaction between the whole system allows them to move forward. It may be a challenge because getting directives from an expert, rather than looking within their own system, is what they have come to expect.
Using a Virtual Family Map to Identify Issues in Families
Before talking about the influence of social media on the family, it is important to acknowledge some of the “players” in social media. The system of social media has many parts. Social media success is dependent on an algorithm, which encourages frequent interactions by virtual and non-virtual friends.
The frequent interactions result in the shareholders receiving monetary return on their investment, the employees maintaining their jobs and bonuses, and the advertisers increasing the visibility of their product resulting in increased sales. The influencers are dependent on social media to reach as many people as possible to receive income from the app. There is a lot of pressure to have an effective algorithm to support social media.
As you next look at a map depicting the interactive nature of the family and social media, it is important to keep in mind that the 24 triangles from the non-virtual map are still present, and the family boundary is already disintegrating with the school workers, friends, and therapists to seek help with the identified patient.
Now in addition to these non-virtual professionals and friends, the family is inviting social media’s virtual friends and influencers to seek help with the identified patient. Clients (and non-clients) often turn to virtual friends and influencers to provide the same connection as non-virtual friends, but these connections are void of physical closeness. Children and adolescents believe a virtual relationship can replace a non-virtual relationship. But all virtual relationships are void of physical closeness in which touch, eye contact, and a warm smile can feed the soul.
The family can turn on a social media app at any time of the day or night and the outside world is invited into the family, increasing the number of triangles exponentially. From the clinical perspective, it is critical to examine what actions (social competition, social comparison, loneliness, etc.) in the family trigger a member(s) to invite social media into the family. The therapist must also discuss how social media algorithms are activating/triggering the member(s) of the family to turn to an app to surf or post an event. This increases the time spent on the smartphone to maintain these virtual friends, non-virtual friends, and influencer relationships.
At times, social media decreases connection with non-virtual relationships and increases the connection with virtual friends and influencers. In the therapy session with this particular family, some members discuss how they rely on virtual friends and influencers more because “they understand me more than the friends in my own town/school.”
The adolescent believes these virtual figures want to listen to them more than family and non-virtual friends. It is important to ask the family what influencers and virtual friends provide that their own family members or non-virtual friends cannot. This allows the clinician to address the patterns and interactions in the family.
In the map below, I do not draw the number of different social media apps, influencers and virtual friends who are involved with the family. However, I do recommend when meeting with families, to draw each app, virtual friend, and influencer to show the number of triangles the family is managing or attempting to manage. For simplicity’s sake, I use one (black) box to represent all the social media apps and one box for all influencers and separated mom and son’s virtual friends.

Husband, Wife, and Social Media Triangle
What is the impact of social media on marriage? The wife turns to social media and influencers to figure out how to “fix” her marriage. The wife tries to talk to her husband about what she has learned about marriage on social media. The husband discounts the wife’s attempts to “educate him about marriage.” She eventually gives up on the marriage and “wants to focus more” on her son. She also tries to connect with previous friends and boyfriends from past life because she feels lonely and alone “looking for a connection.”
What you will see in this triangle, and all the triangles which involve social media, is a substitution of a virtual relationship for a non-virtual relationship whose connections are full of conflict or conflict avoidance. The virtual relationships convey an illusion of meaningful connection, but the person(s) feels alone and lonely because it lacks the important ingredients for a fulfilling relationship.
Mother, Father, and Social Media Triangle
Now the wife stops working on the marriage and focuses on parenting. The husband is not aware of this decision, focusing on “making money to provide food, clothing and shelter.” The father continues to feel alienated, disconnected, and disempowered, becoming angry towards the mother and son. The mother turns to school staff, therapists, non-virtual friends, virtual friends, and influencers for ways to “fix her son.”
This fosters more of an enmeshment with son, and disengagement with Dad. The son turns to school staff, his therapist, non-virtual friends, virtual friends, and influencers. Each family member describes a feeling of disconnectedness trying to overcome the feelings of being lonely/alone. Dad voices his frustration, complaining that he is “old school,” and they are “hypnotized by that damn phone.”
Mother, School, and, Social Media Triangle
In this triangle, mom calls the teachers and guidance department for support. She has frequent phone calls with the guidance counselor because the guidance counselor “is an expert with adolescents.” As you can see, dad is left out of the interactions with the school.
After a few months, her son’s behavior is not changing, and mom is frustrated with how the school is not helping her son. Mom begins to turn to social media looking for answers. Mom spends hours on the app talking to non-virtual friends, virtual friends and reading/commenting on influencer’s posts. Mom displaces healthier activities with time spent on social media. Mom begins to complain that the school is not meeting the goals set out by the Individualized Education Plan (IEP). Mom cites information from influencers from social media and the internet. The tension rises between the school and mom.
Schools today are under tremendous pressure to perform. Schools are understaffed, and do not have the mental health training or support to bring in a countercultural systemic approach into the schools despite the money being put into schools after COVID-19.
Parents, Son, and Social Media Triangle
Mom is spending hours on social media looking for answers to why her son is struggling. She also spends time looking for connections. The son also spends hours on the app interacting with non-virtual friends, virtual friends and reading influencers’ posts.
Mom pursues the son, but he only is aligned with her to challenge dad’s limit setting. When the parents attempt to be aligned, the son acts out more. We see the son increase his conflict with parents, who struggle due to their enactment/conflict avoidance with each other on how to help their son. This results in the father leaving and the mother turning to social media to find answers or overcome feelings of loneliness.
When the family interactions are in intense conflict or conflict avoidance, many children, adolescents, and young adults get most of their answers from non-virtual friends, virtual friends and influencer’s posts. The son is seeking temporary relief by getting information and trying to affirm a sense of self.
The non virtual, virtual relationships, and influencers introduce beliefs that are the opposite of the family’s beliefs and further impact the self-esteem of the adolescent. The son discusses what he learns from social media of what “real parents are like.” The decrease in face-to-face communication with family increases his anxiety, depression, irritability, and intrusive thoughts. This also confuses the family of how their family member can “think so differently.”
Son, Non-Virtual Friends, and Social Media Triangle
The son in the session discusses constant social competition/comparison, working for social currency, and thinking he at times is invisible to his non-virtual friends. The son gradually believes his non-virtual friends “don’t understand.” He believes he cannot turn to his parents because “What do they know?!”
The son begins to engage in the same interactions with his peers as his parents and avoids turning to his peers for support. The son begins to spend more time on social media with virtual friends and influencers to seek select information that matches a narrow/closed view, hoping to avoid conflict/interaction. The son then turns more to virtual friends and influencers for answers. Again, this increases his time on his smartphone and increases the family’s sense of not being good enough for each other.
Remember, the son believes there is “less stress” getting information from a stranger, pop culture icon, or a virtual friend than an enmeshed mom, disengaged father, or face-to-face with a peer(s). However, the decrease in face-to-face communication with family and non-virtual friends increases his anxiety, depression, irritability, and intrusive thoughts.
Despite the time spent on social media, the son feels alone/lonely, looking for emotional, face-to-face and physical connection, but does not have the words to express these thoughts to each other.
Mom, Therapist(s), and Social Media Triangle
Dad continues to be absent from the triangle that involves the therapist. The mother attends her own therapy and attends her son’s sessions to discuss what new information she has seen on social media.
She reviews with both therapists what she has learned on social media about new treatment, new medication, and new diagnoses. She advocates with all providers that her son is incorrectly diagnosed, hoping that would help him with his symptoms. The quality of training of the therapist determines their response to entertaining or challenging mom’s research. This may result in mom seeing a new therapist.
The individual therapists and psychiatrists are not looking at how the parents avoid “getting on the same page.” They are reacting to reports by mom about the son’s behavior. Mom and dad are unable to interact differently because they have not figured out how to work together to decrease their son’s phone usage to increase his time with non-virtual friends. The professionals are avoiding addressing the parent’s avoidance!
Mom, Psychiatrist, and Social Media Triangle
Dad is absent from the triangle that involves the psychiatrist. Mom becomes disgruntled with the psychiatrist. She begins to challenge the psychiatrist’s diagnosis and medication recommendation. The psychiatrist recommends if mom is not satisfied with his assessment, she seek a second opinion. Mom begins to look for a psychiatrist who agrees with what she has read on social media.
Son, System of Care, and Social Media
The son is seeing his individual therapist 1-2 times a week and his psychiatrist once a month. He is also spending 2-8 hours on his social app each day. The therapist has not assessed the hours the son is spending on his phone. The app is only showing views/opinions/likes/images that interest him.
The son begins to complain that the therapist does not understand him and challenges his therapist saying, “This doesn’t help.” When the therapist explores the son’s statement, he begins to discuss information from “reliable sources” from social media and influencers. He too begins to diagnose himself and discusses medication that can help. When the system of care discusses reliable sources such as universities and professional journals, the son becomes irritated saying “I don’t want to read them.”
Son, School Staff, and Social Media
Not only does the system of care increase their sessions, but the school staff increase their time with the students. The number of triangles with the son in the school increases between the child study team, teachers, and administration.
The teachers are pursuing him to get his work done — offering to meet him before school, lunchtime, and after school to complete his work. He never shows. The son is seen in class on his phone. Some teachers ignore him, and others nag him. When a teacher challenges the time he is on his phone, he tells the teacher other instructors let him do it.
The social worker is calling him down to discuss his avoidance of work and disruptive behavior in the classroom. Only when the son becomes overwhelmed, he discusses with the school social worker his home life and that medication is not working. The vice principal is meeting with him to give him detentions. The son feels frustrated with the school stating, “They are only doing this because it is their job.”
Son, Non-virtual Friend #1, Non-virtual Friend#2 with Social Media
The son leaves school to go home to continue to work on his non-virtual relationships on social media. It becomes evident that in social media apps, the same social stressors occur online like in school. It is exhausting to navigate being included and avoid being excluded at school and online. The son and non-virtual friends are jockeying for social currency and social position, never getting time off to charge their own social battery.
The son and non-virtual friends stress about the images they post. They are anxious about what the image means to them and others. The son is trying to understand the unspoken rules for posting and the reaction by his peers regarding the image. The son worries if the image appears “authentic” and will help him maintain his position inside the social media group or if a new group be formed without them.
Son, Non-virtual Friend(s), and Virtual Friends
The son struggles connecting with his non-virtual peers. He is not getting feedback from his non-virtual friends about his art and his physical appearance and finds out they have different chat rooms that do not include him. (Remember, he does not want feedback from an overly involved mom or detached father.)
He begins to look for feedback about his art and physical appearance from virtual friends. When looking for connection outside the non-virtual friend group, he states he is looking for virtual friends who are nonjudgmental.
But as time went on, it began to mirror the non-virtual group. Some of his virtual friends on social media become competitive and attempt to increase their social currency on this platform. They do this by making fun of his physical features and his art. This mirrors some of his non-virtual friends’ behavior. The son frantically searches for another virtual peer group that he believes will not activate anxiety by not challenging his views, providing a stress-free venue.
As the son increases his time searching for virtual peers and influencers over non-virtual friends — reinforcing a closed system, increasing isolation at school, and decreasing time to sleep at home. His virtual relationships are now more important — increasing time spent on the app and continuing to strive for more likes and views.
Lack of face-to-face contact with family and non-virtual friends fosters more of a virtual enmeshment with virtual friends. He describes them as “nonjudgmental” and “more accepting.” This further increases his self-doubt and increases his feelings of loneliness and creates a virtually closed system (Virtual Enmeshment).
Son, Virtual Friends, and Influencers
The virtual group is important to maintain when avoiding contact with his parents and non-virtual friends. The son describes his virtual friends as more “authentic” and describes his non-virtual friends as “fake” and “not genuine.” However, some of his virtual friends on social media become competitive and attempt to increase their social currency.
The son frantically looks for another group that is an anxiety and stress-free venue. This further increases his self-doubt and increases his feelings of loneliness. This increases the symptoms of anxiety and depression when waiting for approval from virtual friends saying, “They are the only ones who understand me.”
As the son looks for new virtual friends, he and his virtual (and non-virtual) friends look to influencers for answers on how to portray themselves. Influencers work hard to establish and maintain their position in their virtual community. The influencers are working hard to make money and increase their viewership. The influencers often ask adolescents to agree with their beliefs and recommend products they are selling. The influencers work hard to appear on the “right side” of an issue.
As the son tries to replicate the beliefs of his preferred influencers, he looks for fellow virtual friends that have done the same “research.” They notice the more they make comments in opposition to a belief, it increases their views and likes.
As the symptoms in the family increase in intensity, the members increasingly must decide who to align themselves with in the virtual and non-virtual triangle. The therapist highlights this and encourages the family to discuss and identify the boundaries of virtual and non-virtual triangles that maintain these alliances/symptoms. This allows a family to discuss non-virtual triangles that are underutilized, which reinforce healthy boundaries that benefit the family.
Using Exploring Questions to Make Circular Statements
Much has been written about joining, unbalancing, and mapping in SFT. One of the beautiful ways Structural Family Therapy (SFT) uses language is by employing circular statements to connect the family member’s behavior in the system. When SFT enters the family, the systems therapist uses the family’s own observations to connect their interactions.
It is important today to make a circular statement to widen the lens in which the family sees how all virtual and non-virtual relationships impact the relationship in the family. Below are some examples of circular statements using the words used by each family member.
I agree with you, Mom, that as long as you do not have a voice with Dad and work together, your son will not stop posting explicit images on Snapchat
Dad, as long as you sound like a drill sergeant, Mom will not find her voice as a woman and work with you as a wife and mother of your son who will continue to believe he must mirror images on Instagram
Mom, I agree that the harder you work, the less Dad helps you with parenting your daughter— your daughter will have to turn to influencers about how a woman should look and act
Peter (son), as long as your mom is worried about the frontstage appearance, she will fight with your father who is more concerned about your backstage struggles with you and your mother
What do your virtual friends give you that you cannot get from Mom, Dad, or your non-virtual friends?
Conclusion
Many are worried about the continued increase in suicide, suicide attempts, and mental health issues in the family and how Congress is powerless to challenge these companies. Many providers are not looking at what has changed in our lives in the past 25 years.
Relationships are becoming more complicated than ever. Many families and therapists are unaware of the impact of the system of care and less aware of the impact of the ubiquitous “algorithm.” It is hard to understand how the algorithm works because it is important for these companies to keep the algorithm secret for fear of losing profit.
We must also remember that each influencer, virtual friend, and nonvirtual friend has their own family map. Just as many professionals do, influencers understand how their stories, views, and images echo in the family.
Are families aware of the alliances that occur with virtual and non-virtual friends and influencers? Are we aware that when more virtual influencers and friends enter the family, more alliances increase establishing social hierarchy, increasing social competition and social currency? Are we, the clinicians, aware that influencers and virtual friends unintentionally/intentionally begin to write/rewrite stories in the family and permanently on the internet?
We must begin to understand that with more stories, there are more opposing interests for each family member. This phenomenon between families, virtual friends, nonvirtual friends, and influencers (social media) is a result of collusion when all parties collaborate to uphold their preferred sociocultural trend.
The goal is not only to highlight and interrupt the multi-alliances with existing social media but to highlight the transactional pattern in the home that maintains this pattern. Remember, a virtually closed system impacts all family members, whether one or all are using these platforms excessively.
References
(1) Susruthi, R., Myara, Maymone, B. C. & Vashi, N. Selfies-Living in the era of filtered photographs. JAMA Facial Plastic Surgery. 2018 20:6, 443-444.
(2) Nesi, J. (2022) The impact of social media on youth mental health: Challenges and opportunities. North Carolina Medical Journal, 81(2), 116-121.
(3) Colapinto, J. (1995) Dilution of family process in social services: Implications for treatment of neglectful families. Family Process. 34:59-74.
Questions for Reflections and Discussion
How has social media influenced your personal and family life?
How does the author’s premise resonate with you and the way you practice family therapy?
How have you integrated social media and app use into family therapy?
In what ways do you agree or disagree with the role of social media in family systems?
© Psychotherapy.net 2023

.png)
.png)