
A culturally sensitive therapist connects deeply with an indigenous client, using Narrative Therapy techniques and EMDR to support her in healing herself and her community.
Critical Tips for Building and Maintaining Your Private Practice: Avoiding Self-Defeat
How to successfully build and maintain your private psychotherapy practice by taking a client-centered approach towards your office and communication protocols.
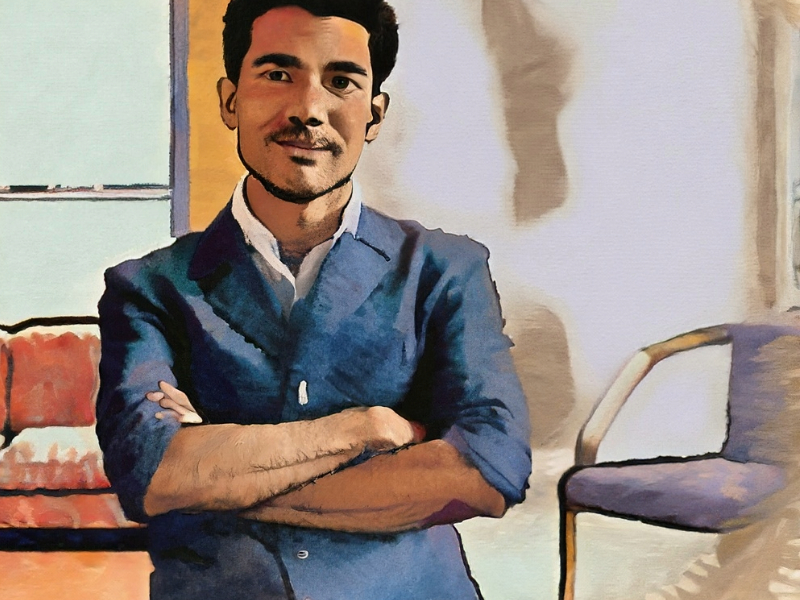
Strengthening the Therapy Relationship with Gay Men
The keys to successful therapy with gay men are connection, support, and attunement. Excerpted from Unwrapped, Integrative Therapy with Gay Men…the Gift of Presence.
The Costs and Benefits of Virtual Reality in Psychotherapy

Therapists considering the role of virtual reality with their clients, particularly the elderly, must carefully consider the costs and benefits.
Stealing a Passage Home: Narrative Therapy to Re-claim Honesty

Kay Ingamells uses playful Narrative Therapy techniques to help a young client regain his honesty.
Using the Filipino Practice of Shared Inner Perception in Psychotherapy

The Filipino practice of Pakikiramdam (shared inner perception) is a valuable tool in psychotherapy, deepening intuition, attunement, collaborative projection, and co-transference.
The Symbolic Healing Power of Traditional Coping Strategies

Adding symbolism to coping strategies can increase your client’s ability to resolve psychological distress.
Katja-Writing: Being Author and Audience to Fictionalized Stories of Trauma- Part II

Join Christoffer Haugaard and David Epston as they deepen and conclude their powerful work with Irene to build stories through which she heals from brutal childhood trauma.
Will Computers Replace Psychotherapists?

The promises of artificial intelligence are profound and wide-reaching. Will those promises include replacing psychotherapists?
Makungu Akinyela on Testimony and the Mattering of Black Therapy
In this riveting interview with scholar and clinician, Makungu Akinyela, we learn the matters of Black therapy and that Black Therapy matters.