Okay Rosenthal, tell me something about psychotherapy I dont know. Fine: I will! If youve read all the textbooks, analyzed the classics, and been to enough workshops to receive frequent flyer miles, Ive got something new to teach you so put down the managed care forms, and pay attention. My secret weapon for improving your psychotherapy sessions comes from the field of copywriting. Thats correct, I said copywriting. Copywriting is the act of creating written documents that persuade customers to reach…
Ethical Guidelines: Do We Really Want What Is Best For Our Clients?
Most therapists are familiar with the affliction of Seasonal Affective Disorder (SAD). SAD impacts approximately seven million people each year in America, mainly women. At one point in my career I shared a private practice office with a psychiatrist. She would use the office on some days and I would use it on others. When I entered the office for the first time I was struck by the fact that she had a phototherapy apparatus in the room. It was physically…
How One Desperate St. Louis Psychotherapist Cured A Schizophrenic
Maggie began the session by telling me that she had been diagnosed by three different psychiatrists. The good news was that all three agreed on the diagnosis. The bad news was that each psychiatrist told her she was schizophrenic. “So, what brings you here today?” I asked. “Well, I saw something in the newspaper and it said you wrote some books on mental health and teach in the field so I thought you might know something these psychiatrists don’t.” (Wow. How refreshing. A…
Interrupting the Conversation: Gestalt Therapy Here and Now
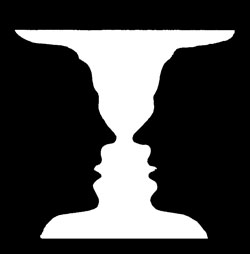
Using a case study with a disconnected client, a contemporary Gestalt therapist debunks myths that have lingered from the heyday of Fritz Perls.
Violet Oaklander on Gestalt Therapy with Children

The founder of Gestalt therapy with children and adolescents discusses therapeutic relationship building with kids and teens, the unique rewards of introducing expressive arts therapy techniques, and the challenges of being sufficiently directive in working with children.
The God of Hellfire Will See You Now

How often does a proto-Goth heavy metal rock star become a psychotherapist?
Robin Rosenberg on Treating Eating Disorders

A psychologist specializing in eating disorders discusses etiology, cultural factors, and treatment options for eating disordered clients and patients.
Sleep and the Therapist: A Poem

A therapist poetically chronicles an underreported occupational hazard.
Supervision of Executive Coaching
Last year I was tempted out of my retirement as a psychotherapist to provide supervision to a group of colleagues working with business executives. This was not psychotherapy but coaching, and my protests that I had never done any coaching or even read very much about it were overruled: they wanted me and they had every confidence that I would do a good job. I was flattered of course, intrigued too, and the extra money was welcome. So I began….
James Gilligan on the Psychology and Treatment of Violent Offenders
Renowned Harvard psychiatrist and violence expert James Gilligan offers insight into working with violent offenders in prison settings. Learn about the tragic childhood origins of violent behavior, as well as the fundamental principles of psychotherapeutic treatment of forensic clients.