Whether it’s the anger-fueled drive that results in the winning goal or the disgust over a ref’s call that ends in a turnover, emotion is almost always present in sports.
The field of sports psychology is relatively young and is comprised of various disciplines such as mental performance, mental health, coaching education and leadership development. As universities are hiring in-house sports psychology practitioners to improve the performance, wellbeing, and leadership of athletes and coaches, high schools across the country are beginning to follow suit. While I continue my journey in the field of counseling psychology as a 4th year doctoral student at UW-Milwaukee, I also help area teams and individuals improve their mental performance through my performance consulting practice.
One of my major clients is a high school in Southeastern Wisconsin, where my role is to work on an integrated team that oversees the 22 sports programs at the school. This team is comprised of an athletic trainer, school counselors, strength and conditioning coaches, head coaches, and administrators. Each part of the team comes in contact with student-athletes to help them improve, and my role as the mental skills coach is to help athletes enhance mental and emotional aspects of training and competition that are sub-clinical in nature. Should elevated risk become apparent, student-athletes are referred to the school counselor.
Following an early season mental skills session with the girls track and field program, an assistant coach approached me with an athlete I had not yet met. Anna, a shotput and discus thrower on the team, asked if I would be willing to work with her to improve her confidence and the mindset she carries into competition.
After we chatted for a bit, it became clear that Anna was looking for two things. First, she directly discussed her lack of self-confidence and asked for help improving it, and secondly, she alluded to an inability to manage her emotions when she was in the throwing ring at competitions.
Throughout the season, Anna and I met during practice to discuss progress made toward becoming more confident when competing. Things seemed to be trending in a positive direction as she was able to improve her self-talk, visualization, and acceptance of things she cannot control, all elements to improving confidence in sports. She was achieving high grades in her advanced-placement courses and was throwing better and better at each meet. While the championship season approached, Anna, like so many other high school athletes, started to doubt her ability to complete a successful season, yet was excited to throw at the upcoming Regional Championships coming.
After throwing a personal best in both shotput and discus at the regional championship, Anna qualified for the sectional championships—a goal she’d had since beginning her athletic career.
Despite having achieved her goal, at the sectional meet Anna seemed to lack the confidence and poise that had become a staple in her competition game plan. She scratched her first throw in discus and under-performed in her next two. With three throws remaining, Anna was feeling the heat. Her coaches continued to give feedback on technique, and finally she came up to the coach’s box where I was watching her throw.
“You look really angry, and your body language is showing it,” I said. This was a tone not typical in my repertoire, yet the situation called for a direct approach as time was an imminent factor.
“Yeah, my first three throws were horrible and I’m not going to make it to state,” she responded.
“Has being angry been helping?”
“No.”
“Has telling yourself you’re not going to make it to state been helping?”
“No.”
“Am I way out of line to think that maybe we need to try something new?”
“No.”
“How can we manage our anger right now?”
“Let it go?”
“Yes! We’ve been working on a lot of breathing and that may help but find a way to bring your anger down a little during these next few throws and let’s go from there.”
“Alright, yeah, that sounds good.”
Anna closed her eyes, focused on her breath, and looked visibly more relaxed heading into the next few throws. She qualified for the state meet on her fifth throw, delivering a new personal record in discus. Carrying her relief into shotput, Anna set another personal record to qualify in her second event.
Two weeks later, after setting a new discus school record at the state championship and the largest stage of her career, Anna sat in the stands discussing her progression throughout the season.
“I just got in the ring and relaxed,” she said. “I don’t know, I just let it go.”
As the mental skills coach, I could not have been prouder.
My joy for Anna didn’t come from some sort of vicarious experience through her state championship run and school record toss, but rather in her ability to acknowledge her areas for growth, seek out someone to help, and engage in the journey to improve. The end result was the product of intrinsic motivation and facing up to vulnerability week in and week out.
Not once did Anna need to “calm down” nor was she ever told that her emotions were “getting in the way” It wasn’t implied by anyone who she trusted to work with. Instead, she was empowered by her coaching staff to find ways to manage what she was experiencing and go after her goals with all she had. She was tough, and her fighting spirit shone through in the good times and the bad.
No matter how you identify or what you do, emotions are not inherently bad. They’re just a piece of the puzzle that can be analyzed, managed, and at times, utilized. Anna was encouraged to strive for more, but not at the cost of her self-identity or personal values. She showed up on the biggest athletic stage in her career and found success by sticking to her values and game plan; and having a little fun along the way.


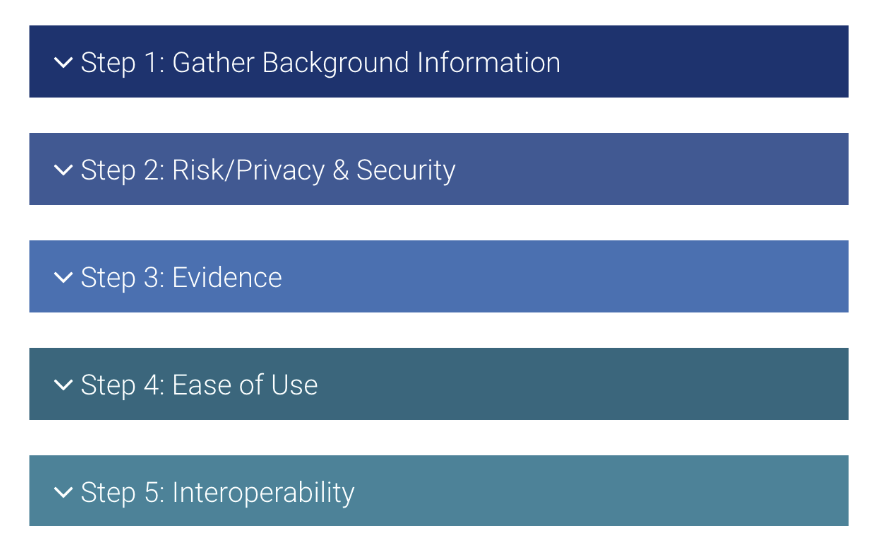 On the other hand, technology can be an important tool in our work. For my children and adolescent patients, using apps to track mood and sleep have yielded more cooperation than tracking those metrics on paper. Apps that track mood and anxiety symptoms can help individuals share their symptoms with their doctor or therapist. As professionals, we can guide our patients in choosing apps that best meet their needs. Apps are not regulated and there is little oversight into their creation or claims. We can help our patients become better equipped to choose apps that are helpful rather than harmful. The American Psychiatric Association has created guidelines to assist professionals in helping individuals choose the best mental health related apps. The APA has developed the App Evaluation Model that can help providers evaluate the appropriateness of an app with their patients. (see figure)
On the other hand, technology can be an important tool in our work. For my children and adolescent patients, using apps to track mood and sleep have yielded more cooperation than tracking those metrics on paper. Apps that track mood and anxiety symptoms can help individuals share their symptoms with their doctor or therapist. As professionals, we can guide our patients in choosing apps that best meet their needs. Apps are not regulated and there is little oversight into their creation or claims. We can help our patients become better equipped to choose apps that are helpful rather than harmful. The American Psychiatric Association has created guidelines to assist professionals in helping individuals choose the best mental health related apps. The APA has developed the App Evaluation Model that can help providers evaluate the appropriateness of an app with their patients. (see figure)